

Consultative meeting to develop a strategy for treatment of cutaneous leishmaniasis. Institute Pasteur, Paris. 13-15 June, 2006
- PMID: 17456237
- PMCID: PMC1868746
- DOI: 10.1186/1475-9292-6-3
Consultative meeting to develop a strategy for treatment of cutaneous leishmaniasis. Institute Pasteur, Paris. 13-15 June, 2006
Abstract
Background: A meeting was organized by Drugs for Neglected Diseases initiative (DNDi) and the Institute Pasteur (IP), Paris, to review the treatment for all forms of cutaneous leishmaniasis (CL) and to propose a strategy for the development of new efficacious and affordable treatments.
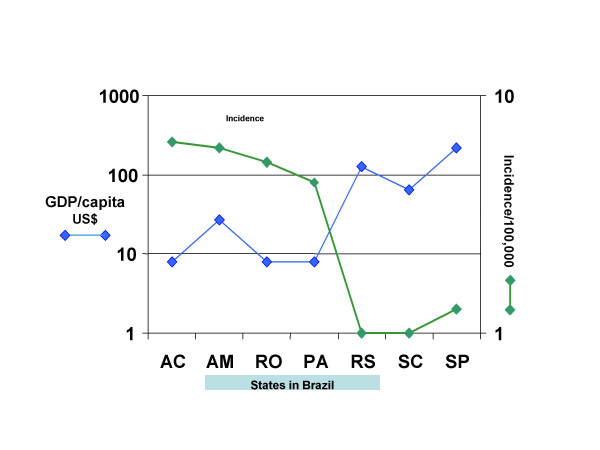
Method: The global burden of CL was discussed with respect to financial impact; relation to poverty; the stigma of CL lesions and scars (particularly in young women); lack of effective, affordable, easily implemented tools and political will and resources to implement available control tools; and lack of input from pharmaceutical and biotechnology companies to develop new drugs and vaccines.
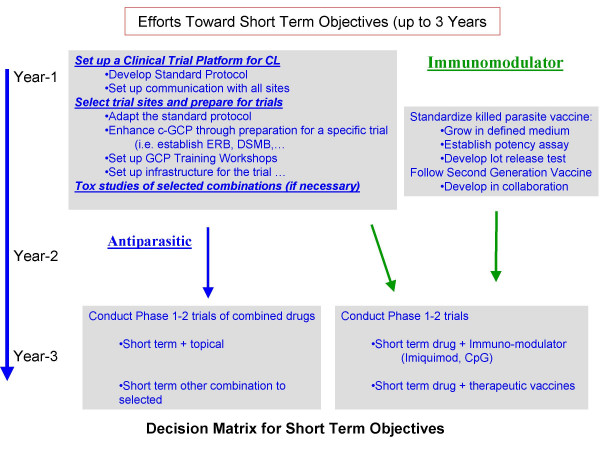
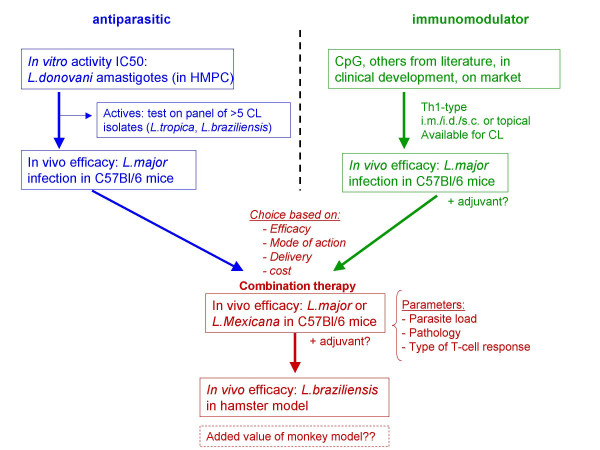
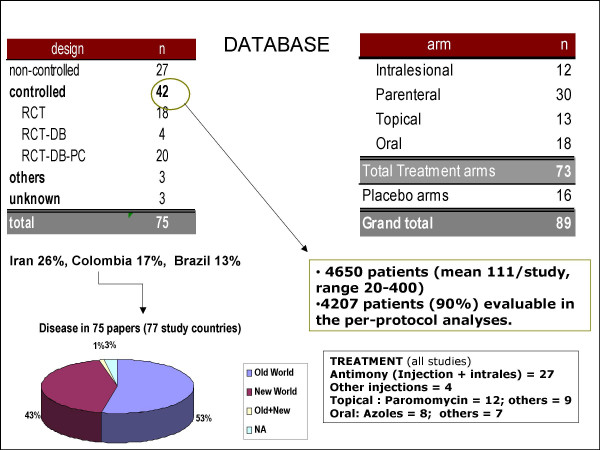
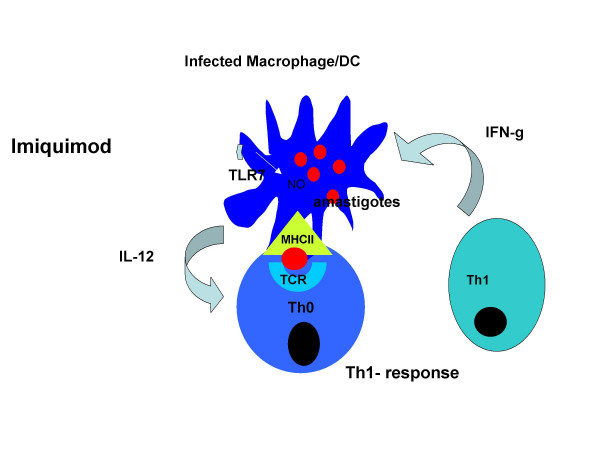
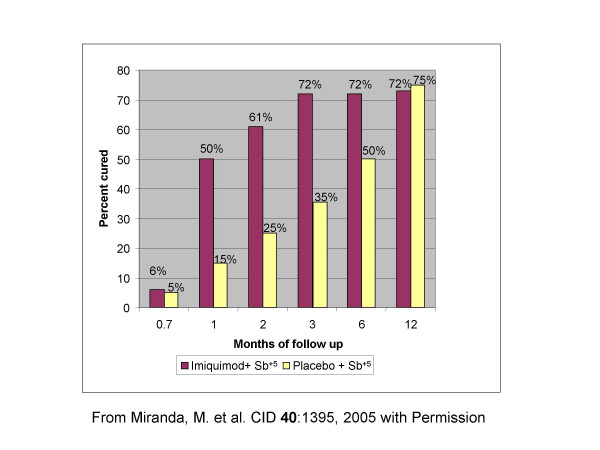
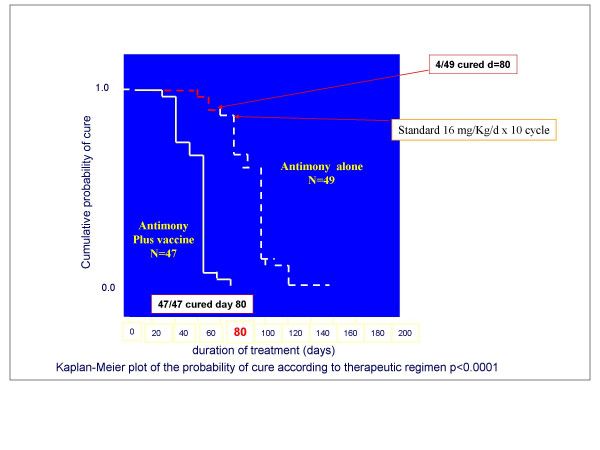
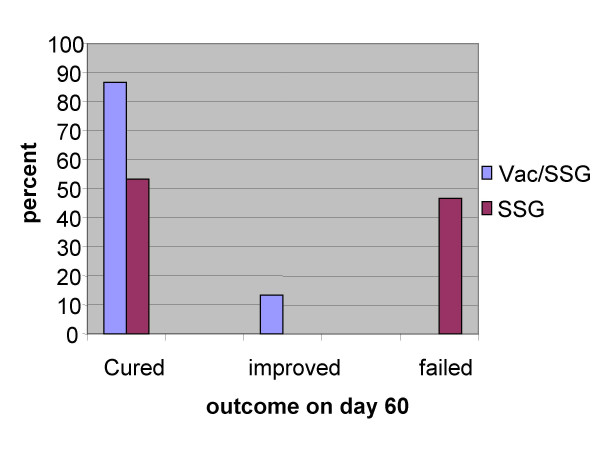
Results: According to the experts from different endemic countries present, the financial and social burdens of CL are high, but we have limited quantitative data. The analysis of published trials indicates that the quality of most trials is poor and requires both improvement and standardization. The available drugs are inadequate. Criteria by which different CL types could be prioritized as target disease were set. These criteria included: severity of the disease; lack of response to available drugs; overall incidence and prevalence of the disease; sequelae of the disease, (including recidivans and mucosal leishmaniasis); the impact of treatment of individuals on control of transmission and lack of other major parties involved in drug development. Based on these, the anthroponotic CL and its sequel "recidivans" caused by L. tropica and CL caused by L. braziliensis and its sequel, mucosal leishmaniasis were considered to be the target diseases. The mechanism for controlling Leishmania infection to reach a stable self healing process is a balanced immune response. Immune stimulation during chemotherapy can enhance cure. There is no adequately effective vaccine, but some encouraging results have been obtained with whole killed Leishmania parasites or imiquimod (an immuno-modulator) plus antimonials. Further studies are needed. One safety/immunogenicity clinical trial is currently ongoing with a Second Generation Vaccine (SGV).
Conclusions and recommendations: There is an urgent need for new treatments for all CL types. CL should be considered as a neglected disease and organizations, such as DNDi, should include it in their list of target diseases. It was agreed that immuno-chemotherapy (with "therapeutic" vaccines or immunomodulators) has a strong potential to make an impact as a new therapy of CL with the view of shortening/reducing duration and dose of drug treatment and preventing resistance. There is also a need for safe, affordable and efficacious new chemotherapeutics. The quality of clinical trials needs to be enhanced and standardized. Short and long-term objectives and activities were defined as a part of meeting recommendations.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
