

Evaluation of genetic factors for warfarin dose prediction
- PMID: 17456829
- PMCID: PMC1855340
- DOI: 10.3121/cmr.2007.724
Evaluation of genetic factors for warfarin dose prediction
Erratum in
- Clin Med Res. 2007 Jun;5(2):142
Abstract
Objectives: Warfarin is a commonly prescribed anticoagulant drug used to prevent thromboses that may arise as a consequence of orthopedic and vascular surgery or underlying cardiovascular disease. Warfarin is associated with a notoriously narrow therapeutic window where small variations in dosing may result in hemorrhagic or thrombotic complications. To ultimately improve dosing of warfarin, we evaluated models for stable maintenance dose that incorporated both clinical and genetic factors.
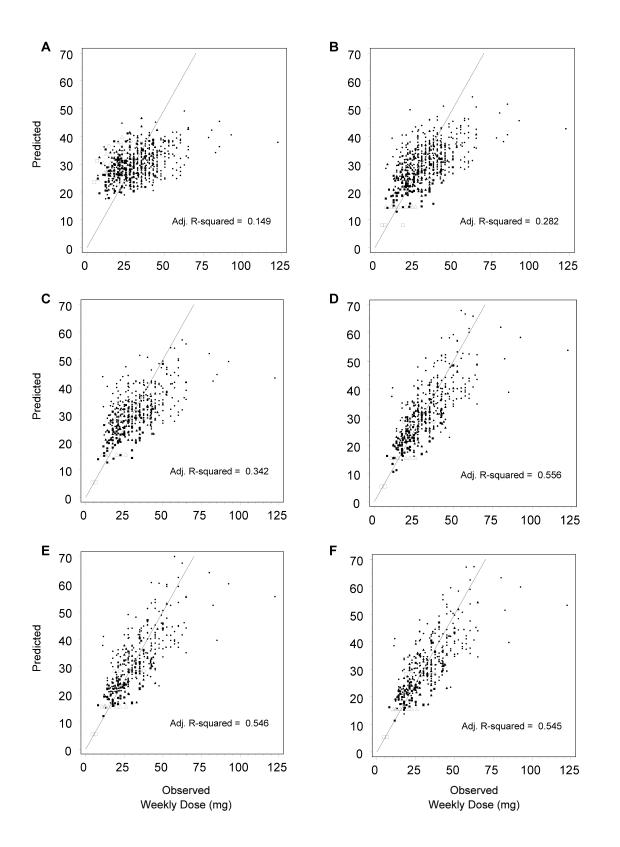
Method: A model was constructed by evaluating the contribution to dosing variability of the following clinical factors: age, gender, body surface area, and presence or absence of prosthetic heart valves or diabetes. The model was then sequentially expanded by incorporating polymorphisms of cytochrome P450 (CYP) 2C9; vitamin K 2,3 epoxide reductase complex, subunit 1 (VKORC1); gamma carboxylase; factor VII; and apolipoprotein (Apo) E genes.
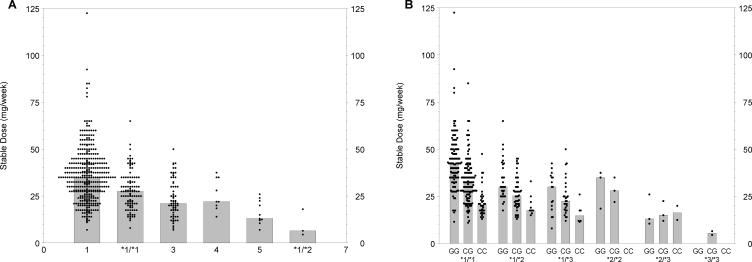
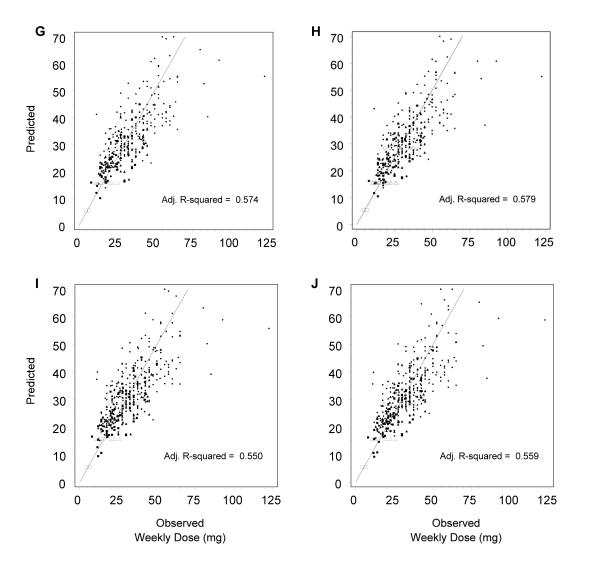
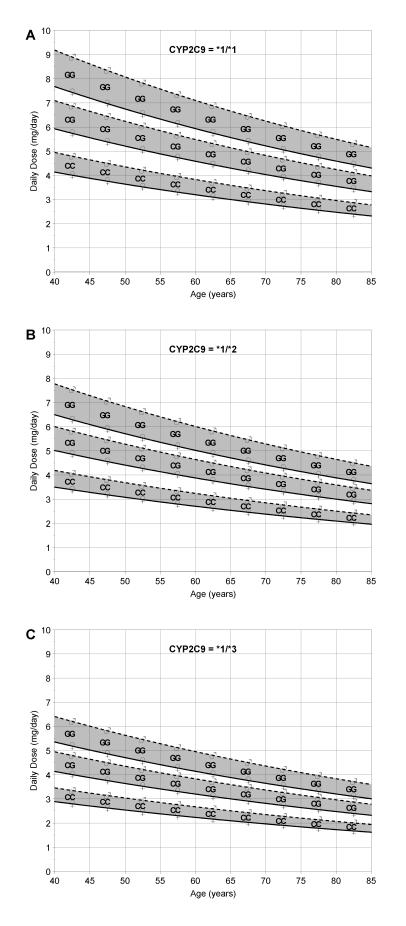
Results: Of genetic factors evaluated in the model, CYP2C9 and VKORC1 each contributed substantially to dose variability, and together with clinical factors explained 56% of the individual variability in stable warfarin dose. In contrast, gamma carboxylase, factor VII and Apo E polymorphisms contributed little to dose variability.
Conclusion: The importance of CYP2C9 and VKORC1 to patient-specific dose of warfarin has been confirmed, while polymorphisms of gamma carboxylase, factor VII and Apo E genes did not substantially contribute to predictive models for stable warfarin dose.
Figures
References
-
- Hardwick ME, Colwell CW Jr. Advances in DVT prophylaxis and management in major orthopaedic surgery. Surg Technol Int 2004;12:265–268. - PubMed
-
- Wittkowsky AK. Effective anticoagulation therapy: defining the gap between clinical studies and clinical practice. Am J Manag Care 2004;10(10 suppl):S297–306. - PubMed
-
- Gutt CN, Oniu T, Wolkener F, Mehrabi A, Mistry S, Buchler MW. Prophylaxis and treatment of deep vein thrombosis in general surgery. Am J Surg 2005;189:14–22. - PubMed
-
- Evans A, Davis S, Kilpatrick C, Gerraty R, Campbell D, Greenberg P. The morbidity related to atrial fibrillation at a tertiary centre in one year: 9.0% of all strokes are potentially preventable. J Clin Neurosci 2002;9:268–272. - PubMed
-
- Caro JJ. An economic model of stroke in atrial fibrillation: the cost of suboptimal oral anticoagulation. Am J Manag Care 2004;10(14 suppl):S451–458. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases