

Lessons from BRCA: the tubal fimbria emerges as an origin for pelvic serous cancer
- PMID: 17456833
- PMCID: PMC1855333
- DOI: 10.3121/cmr.2007.702
Lessons from BRCA: the tubal fimbria emerges as an origin for pelvic serous cancer
Abstract
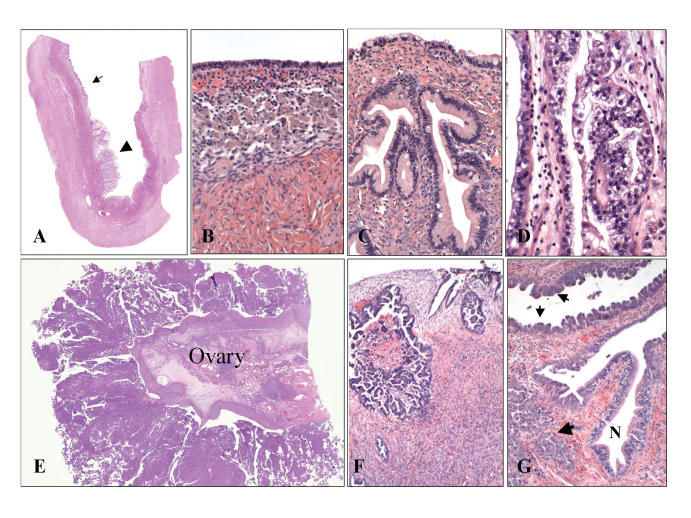
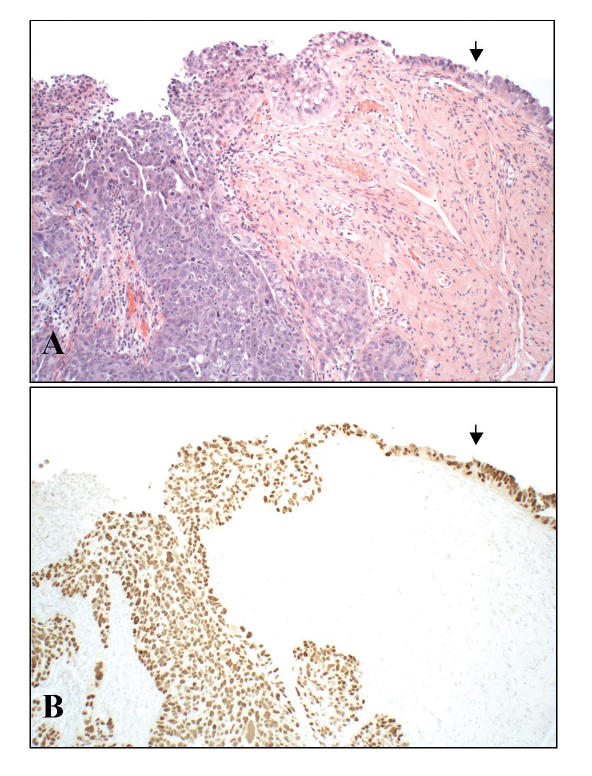
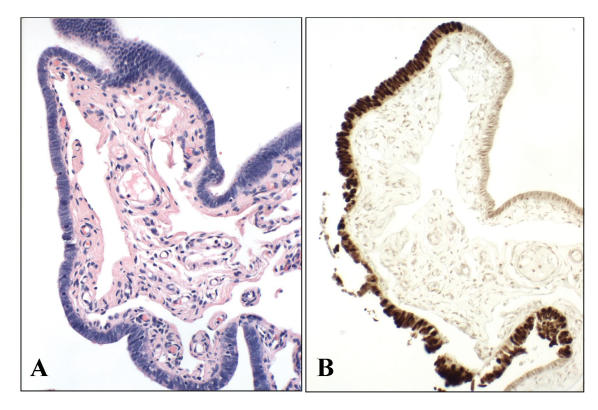
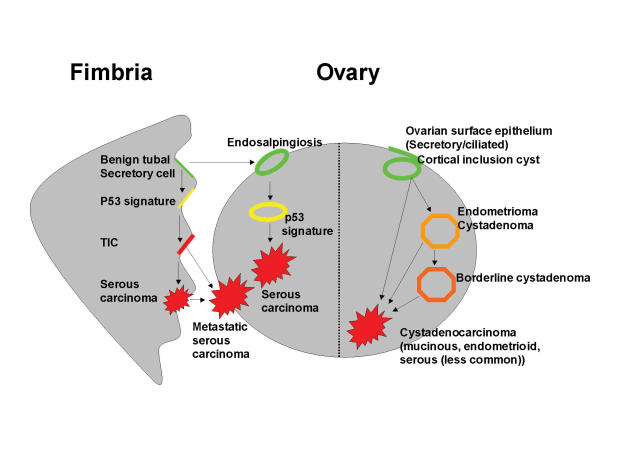
Ovarian epithelial cancer is diagnosed in approximately 25,000 women yearly in the United States, accounting for approximately 12,500 deaths. Of these tumors, serous cancer is the most lethal, due to its capacity to spread beyond the reproductive tract and involve the peritoneal surfaces or distant organs. Conventional classification systems designate tumor origins principally on the location of the largest tumor. However, despite the fact that the largest tumors typically involve the ovaries, demonstrations of a precise starting point for these tumors, including precursor lesions, have been inconsistent. In recent years, a major effort to prevent serous cancer in genetically susceptible women with mutations in BRCA1 or BRCA2 has spawned the practice of prophylactic salpingo-oophorectomy. This practice has surprisingly revealed that many early cancers in these women arise in the fallopian tube, and further studies have pinpointed the distal (fimbrial) portion as the most common site of origin. Emerging studies that carefully examine the fallopian tubes suggest a high frequency of early cancer in the fimbria in unselected women with ovarian and peritoneal serous carcinoma, raising the distinct possibility that a significant proportion of these tumors have a fimbrial origin. The evidence for these discoveries and their relevance to serous cancer classification, early detection and prevention are addressed in this review. A model for pelvic serous cancer is proposed that takes into account five distinct variables which ultimately impact on origin and tumor distribution: (1) location of target epithelium, (2) genotoxic stress, (3) type of epithelium, (4) mitigating genetic factors, and (5) tumor spread pattern. Ultimately, this model illustrates the importance of identifying cancer precursors, inasmuch as these entities are useful as both surrogate endpoints for their respective malignancies in epidemiologic studies and natural targets for cancer prevention.
Figures
References
-
- Quirk JT, Natarajan N, Mettlin CJ. Age-specific ovarian cancer incidence rate patterns in the United States. Gynecol Oncol 2005;99:248–250. - PubMed
-
- Armstrong DK, Bundy B, Wenzel L, Huang HQ, Baergen R, Lele S, Copeland LJ, Walker JL, Burger RA; Gynecologic Oncology Group. Intraperitoneal cisplatin and paclitaxel in ovarian cancer. N Engl J Med 2006;354:34–43. - PubMed
-
- Palma M, Ristori E, Ricevuto E, Giannini G, Gulino A. BRCA1 and BRCA2: the genetic testing and the current management options for mutation carriers. Crit Rev Oncol Hematol 2006;57:1–23. - PubMed
-
- Lux MP, Fasching PA, Beckmann MW. Hereditary breast and ovarian cancer: review and future perspectives. J Mol Med 2006;84:16–28. - PubMed
-
- Sogaard M, Kjaer SK, Gayther S. Ovarian cancer and genetic susceptibility in relation to the BRCA1 and BRCA2 genes. Occurrence, clinical importance and intervention. Acta Obstet Gynecol Scand 2006;85:93–105. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous