

Long-term outcomes following neoadjuvant chemoradiotherapy for esophageal cancer
- PMID: 17457163
- PMCID: PMC1877071
- DOI: 10.1097/01.sla.0000254367.15810.38
Long-term outcomes following neoadjuvant chemoradiotherapy for esophageal cancer
Abstract
Objective: We present and analyze long-term outcomes following multimodal therapy for esophageal cancer, in particular the relative impact of histomorphologic tumor regression and nodal status.
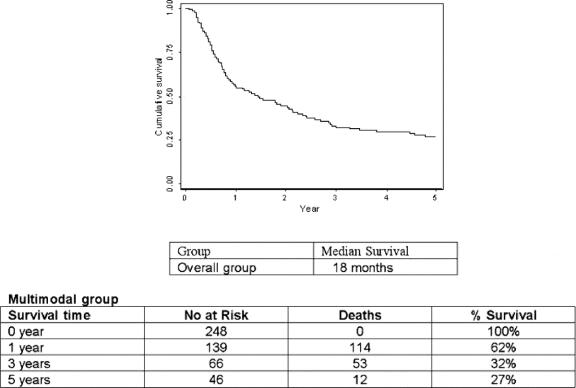
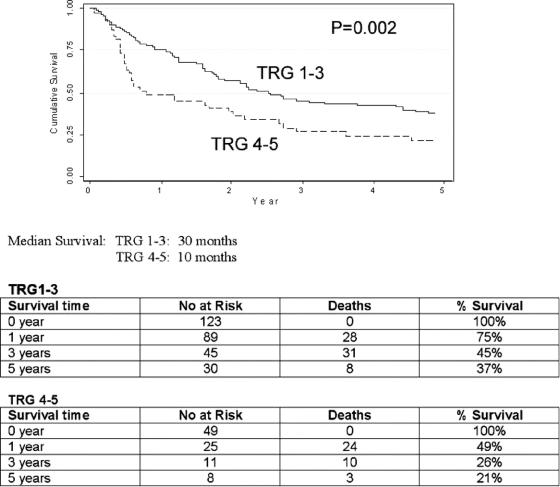
Patients and methods: A total of 243 patients [(adenocarcinoma (n = 170) and squamous cell carcinoma (n = 73)] treated with neoadjuvant chemoradiotherapy in the period 1990 to 2004 were followed prospectively with a median follow-up of 60 months. Pathologic stage and tumor regression grade (TRG) were documented, the site of first failure was recorded, and Kaplan-Meier survival curves were plotted.
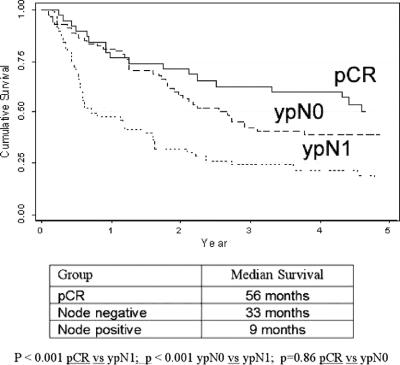
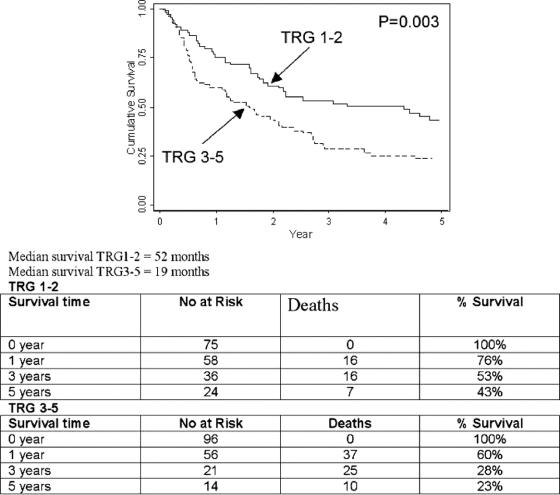
Results: Thirty patients (12%) did not undergo surgery due to disease progression or deteriorated performance status. Forty-one patients (19%) had a complete pathologic response (pCR), and there were 31(15%) stage I, 69 (32%) stage II, and 72 (34%) stage III cases. The overall median survival was 18 months, and the 5-year survival was 27%. The 5-year survival of patients achieving a pCR was 50% compared with 37% in non-pCR patients who were node-negative (P = 0.86). Histomorphologic tumor regression was not associated with pre-CRT cTN stage but was significantly (P < 0.05) associated with ypN stage. By multivariate analysis, ypN status (P = 0.002) was more predictive of overall survival than TRG (P = 0.06) or ypT stage (P = 0.39).
Conclusion: Achieving a node-negative status is the major determinant of outcome following neoadjuvant chemoradiotherapy. Histomorphologic tumor regression is less predictive of outcome than pathologic nodal status (ypN), and the need to include a primary site regression score in a new staging classification is unclear.
Figures
References
-
- Enzinger PC, Mayer RJ. Esophageal cancer. N Engl J Med. 2003;349:2241–2252. - PubMed
-
- Daly JM. Esophageal cancer: results of an American College of Surgeons Patient Care Evaluation Study. J Am Coll Surg. 2000;190:562–572. - PubMed
-
- Blot WJ, De Vesa SS, Kneller RW, et al. Rising incidence of adenocarcinoma of the oesophagus and gastric cardia. JAMA. 1991;265:1287–1289. - PubMed
-
- Pera M, Cameron A, Trastek V, et al. Increasing incidence of adenocarcinoma of the esophagus and eosphagogastric junction. Gastroenterology. 1993;104:510–513. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
