

Is the increasing rate of local excision for stage I rectal cancer in the United States justified?: a nationwide cohort study from the National Cancer Database
- PMID: 17457165
- PMCID: PMC1877081
- DOI: 10.1097/01.sla.0000252590.95116.4f
Is the increasing rate of local excision for stage I rectal cancer in the United States justified?: a nationwide cohort study from the National Cancer Database
Abstract
Objective: Determine rates of local excision (LE) over time, and test the hypothesis that LE carries increased oncologic risks but reduced perioperative morbidity when compared with standard resection (SR).
Summary background data: Despite the lack of level I/level II evidence supporting its oncologic adequacy, LE is performed for stage I rectal cancer.
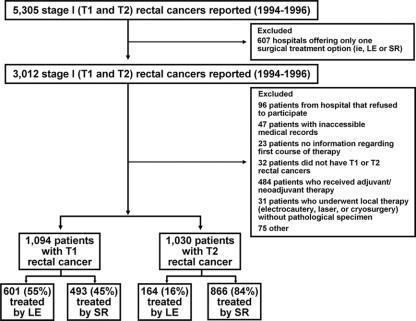
Methods: Surgical therapy for 35,179 patients with stage I rectal cancer diagnosed in 1989 to 2003 was examined over time, utilizing the National Cancer Database. A special study then analyzed perioperative outcomes, local recurrence and survival in 2124 patients diagnosed between 1994 and 1996, including 765 (T1, 601; T2, 164) treated by LE and 1359 (T1, 493; T2, 866) treated by SR.
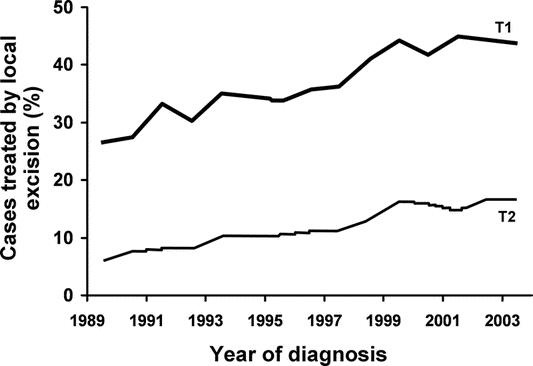
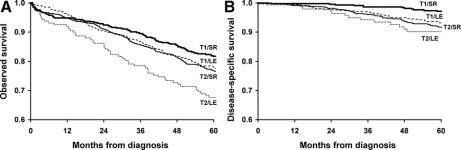
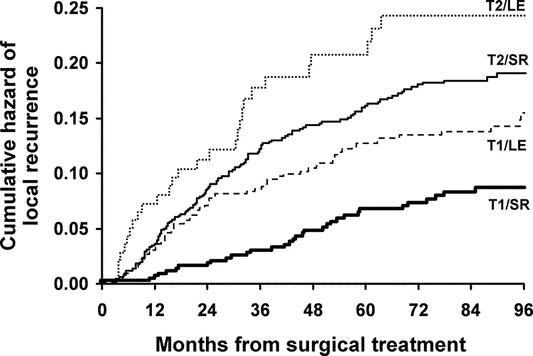
Results: From 1989 to 2003, the use of LE has increased (T1, 26.6-43.7%; T2, 5.8-16.8%; P < 0.001 both). The special study demonstrated significantly lower 30-day morbidity after LE versus SR (5.6% vs. 14.6%; P < 0.001). After adjusting for patient and tumor characteristics, the 5-year local recurrence after LE versus SR was 12.5 versus 6.9% (P = 0.003; hazard ratio = 0.38; 95% CI, 0.23-0.62) for T1 tumors, and 22.1 versus 15.1% (P = 0.01; hazard ratio = 0.69; 95% CI, 0.44-1.07) for T2 tumors. The 5-year overall survival (T1, 77.4% vs. 81.7%, P = 0.09; T2, 67.6% vs. 76.5%, P = 0.01) was influenced by age and comorbidities but not the type of surgery.
Conclusions: This study provides the best evidence for both the increasing use and the associated risks of LE versus SR. For each individual patient, the benefits of LE must be balanced against the heightened risk of local failure.
Figures
References
-
- Ota DM, Jacobs L, Kuvshinoff B. Rectal cancer: the sphincter-sparing approach. Surg Clin North Am. 2002;82:983–993. - PubMed
-
- Bleday R. Local excision of rectal cancer. World J Surg. 1997;21:706–714. - PubMed
-
- Nelson H, Petrelli N, Carlin A, et al. Guidelines 2000 for colon and rectal cancer surgery. J Natl Cancer Inst. 2001;93:583–596. - PubMed
-
- Heriot AG, Grundy A, Kumar D. Preoperative staging of rectal carcinoma. Br J Surg. 1999;86:17–28. - PubMed
-
- Rectal Cancer. Clinical practice guidelines in oncology: National Comprehensive Cancer Network.; Version 2, 2006. Available at www.nccn.org. Accessed June 15, 2006.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
