

Endogenous endotoxin participates in causing a panenteric inflammatory ileus after colonic surgery
- PMID: 17457166
- PMCID: PMC1877055
- DOI: 10.1097/01.sla.0000255595.98041.6b
Endogenous endotoxin participates in causing a panenteric inflammatory ileus after colonic surgery
Abstract
Objective: To investigate muscularis inflammation and endogenous endotoxin as causes of postoperative ileus.
Background: Postoperative inflammatory ileus of the colon is associated with a significant delay in gastrointestinal transit. We investigated whether these changes are caused by the downstream obstructive barrier of the surgically altered colon or by small intestinal muscularis inflammation itself. Furthermore, we evaluated the mechanistic role of gut derived endotoxin in the development of postoperative intestinal dysfunction.
Methods: Rats underwent surgical manipulation of the colon. Isolated gastrointestinal transit was analyzed in animals with ileostomy. The perioperative emigration of intracolonic particles was investigated by colonic luminal injection of fluorescently labeled LPS and microspheres. Mediator mRNA induction was quantified by real-time RT-PCR. Muscularis leukocytic infiltrates were characterized. In vitro circular muscle contractility was assessed in a standard organ bath.
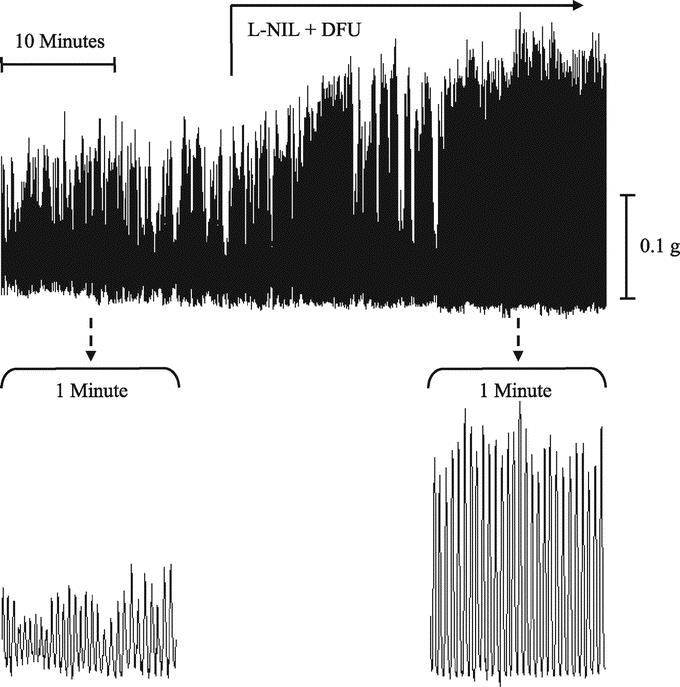
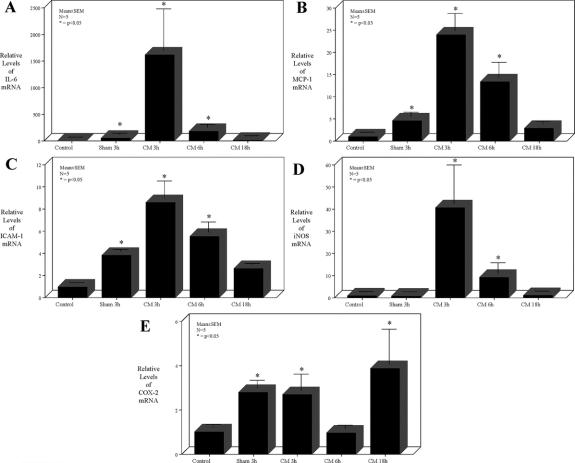
Results: Ileostomy rats presented with a significant delay in small intestinal transit after colonic manipulation. This was associated with leukocyte recruitment and inflammatory mediator mRNA induction within the small intestinal muscularis. Colonic manipulation caused the transference of intracolonic LPS and microspheres into the intestinal muscularis. Postoperative in vitro small intestinal circular muscle contractility was impaired by 42% compared with controls. Gut decontamination and TLR-4 deletion significantly alleviated the small intestinal muscularis inflammation and prevented intestinal muscle dysfunction.
Conclusions: Selective colonic manipulation initiates a distant inflammatory response in the small intestinal muscularis that contributes to postoperative ileus. The data provide evidence that gut-derived bacterial products are mechanistically involved in the initiation of this remote inflammatory cascade.
Figures






Similar articles
-
Colonic postoperative inflammatory ileus in the rat.Ann Surg. 2002 Jul;236(1):56-66. doi: 10.1097/00000658-200207000-00010. Ann Surg. 2002. PMID: 12131086 Free PMC article.
-
Mechanisms of polymicrobial sepsis-induced ileus.Am J Physiol Gastrointest Liver Physiol. 2004 Sep;287(3):G685-94. doi: 10.1152/ajpgi.00359.2003. Am J Physiol Gastrointest Liver Physiol. 2004. PMID: 15331356
-
Selective jejunal manipulation causes postoperative pan-enteric inflammation and dysmotility.Gastroenterology. 2004 Jan;126(1):159-69. doi: 10.1053/j.gastro.2003.10.060. Gastroenterology. 2004. PMID: 14699497
-
Mentation on the immunological modulation of gastrointestinal motility.Neurogastroenterol Motil. 2008 May;20 Suppl 1:81-90. doi: 10.1111/j.1365-2982.2008.01105.x. Neurogastroenterol Motil. 2008. PMID: 18402645 Review.
-
Ileus in critical illness: mechanisms and management.Curr Opin Crit Care. 2002 Apr;8(2):152-7. doi: 10.1097/00075198-200204000-00011. Curr Opin Crit Care. 2002. PMID: 12386517 Review.
Cited by
-
Inflammatory responses in the muscle coat of stomach and small bowel in the postoperative ileus model of guinea pig.Yonsei Med J. 2013 Nov;54(6):1336-41. doi: 10.3349/ymj.2013.54.6.1336. Yonsei Med J. 2013. PMID: 24142636 Free PMC article.
-
Risk factors for postoperative ileus.J Korean Surg Soc. 2011 Oct;81(4):242-9. doi: 10.4174/jkss.2011.81.4.242. Epub 2011 Oct 28. J Korean Surg Soc. 2011. PMID: 22111079 Free PMC article.
-
Effect of the gut microbiota and their metabolites on postoperative intestinal motility and its underlying mechanisms.J Transl Med. 2023 May 26;21(1):349. doi: 10.1186/s12967-023-04215-2. J Transl Med. 2023. PMID: 37237321 Free PMC article. Review.
-
Enteric circular muscle dysfunction in the cystic fibrosis mouse small intestine.Neurogastroenterol Motil. 2010 Mar;22(3):341-e87. doi: 10.1111/j.1365-2982.2009.01418.x. Epub 2009 Oct 8. Neurogastroenterol Motil. 2010. PMID: 19814773 Free PMC article.
-
Neutralizing gut-derived lipopolysaccharide as a novel therapeutic strategy for severe leptospirosis.Elife. 2024 May 31;13:RP96065. doi: 10.7554/eLife.96065. Elife. 2024. PMID: 38818711 Free PMC article.
References
-
- Prasad M, Matthews JB. Deflating postoperative ileus. Gastroenterology. 1999;117:489–492. - PubMed
-
- Chen HH, Wexner SD, Iroatulam AJ, et al. Laparoscopic colectomy compares favorably with colectomy by laparotomy for reduction of postoperative ileus. Dis Colon Rectum. 2000;43:61–65. - PubMed
-
- Piskun G, Kozik D, Rajpal S, et al. Comparison of laparoscopic, open, and converted appendectomy for perforated appendicitis. Surg Endosc. 2001;15:660–662. - PubMed
-
- Maxwell-Armstrong CA, Robinson MH, Scholefield JH. Laparoscopic colorectal cancer surgery. Am J Surg. 2000;179:500–507. - PubMed
-
- Livingston EH, Passaro EP Jr. Postoperative ileus. Dig Dis Sci. 1990;35:121–132. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
