

Hospital volume and late survival after cancer surgery
- PMID: 17457171
- PMCID: PMC1877074
- DOI: 10.1097/01.sla.0000252402.33814.dd
Hospital volume and late survival after cancer surgery
Abstract
Context: Although hospital procedure volume is clearly related to operative mortality with many cancer procedures, its effect on late survival is not well characterized.
Objective: To examine relationships between hospital volume and late survival after different types of cancer resections.
Design: Using the national Surveillance Epidemiology and End Results (SEER)-Medicare linked database (1992-2002), we identified all patients undergoing major resections for lung, esophageal, gastric, pancreatic, colon, and bladder cancer (n = 64,047). Relationships between hospital volume and survival were assessed using Cox proportional hazards models, adjusting for patient characteristics and use of adjuvant radiation and chemotherapy.
Study participants: U.S. Medicare patients residing in SEER regions.
Main outcome measures: 5-year survival.
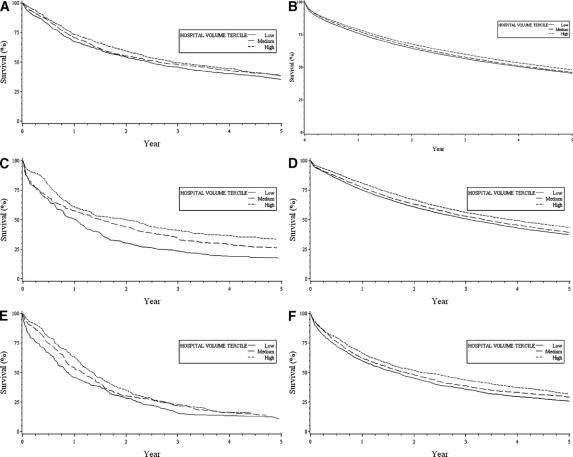
Results: Although there were statistically significant relationships between hospital volume and 5-year survival with all 6 cancer types, the relative importance of volume varied markedly. Absolute differences in 5-year survival probabilities rates between low-volume hospitals (LVHs) and high-volume hospitals (HVHs) ranged from 17% for esophageal cancer resection (17% vs. 34%, respectively) to only 3% for colon cancer resection (45% vs. 48%). Absolute differences in 5-year survival between LVHs and HVHs fell between these ranges for lung (6%), gastric (6%), pancreatic (5%), and bladder cancer (4%). Volume-related differences in late survival could not be attributed to differences in rates of adjuvant therapy.
Conclusions: Along with lower operative mortality, HVHs have better late survival rates with selected cancer resections than their lower-volume counterparts. Mechanisms underlying their better outcomes and thus opportunities for improvement remain to be identified.
Figures
References
-
- Birkmeyer JD, Siewers AE, Finlayson EVA, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128–1137. - PubMed
-
- Begg CB, Cramer LD, Hoskins WJ, et al. Impact of hospital volume on operative mortality for major cancer surgery. JAMA. 1998;280:1747–1751. - PubMed
-
- Dudley RA, Johansen KL, Brand R, et al. Selective referral to high volume hospitals: estimating potentially avoidable deaths. JAMA. 2000;283:1159–1166. - PubMed
-
- Halm EA, Lee C, Chassin MR. Is volume related to outcome in health care? A systematic review and methodologic critique of the literature. Ann Intern Med. 2002;137:511–520. - PubMed
-
- Killeen SD, O'Sullivan MJ, Coffey JC, et al. Provider volume and outcomes for oncological procedures. Br J Surg. 2005;92:389–402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
