

Acute traumatic coagulopathy: initiated by hypoperfusion: modulated through the protein C pathway?
- PMID: 17457176
- PMCID: PMC1877079
- DOI: 10.1097/01.sla.0000256862.79374.31
Acute traumatic coagulopathy: initiated by hypoperfusion: modulated through the protein C pathway?
Abstract
Objectives: Coagulopathy following major trauma is conventionally attributed to activation and consumption of coagulation factors. Recent studies have identified an acute coagulopathy present on admission that is independent of injury severity. We hypothesized that early coagulopathy is due to tissue hypoperfusion, and investigated derangements in coagulation associated with this.
Methods: This was a prospective cohort study of major trauma patients admitted to a single trauma center. Blood was drawn within 10 minutes of arrival for analysis of partial thromboplastin and prothrombin times, prothrombin fragments 1+2, fibrinogen, thrombomodulin, protein C, plasminogen activator inhibitor-1, and D-dimers. Base deficit (BD) was used as a measure of tissue hypoperfusion.
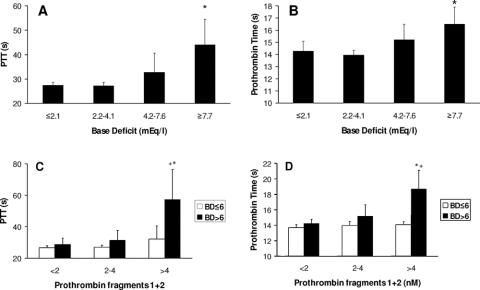
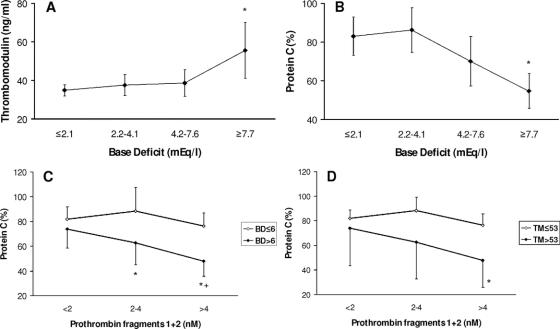
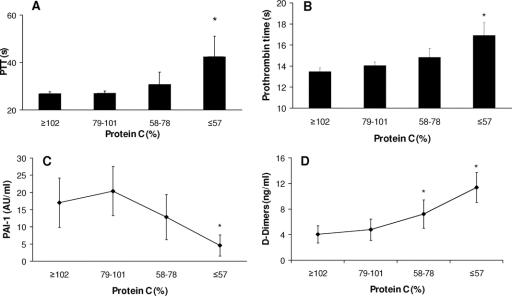
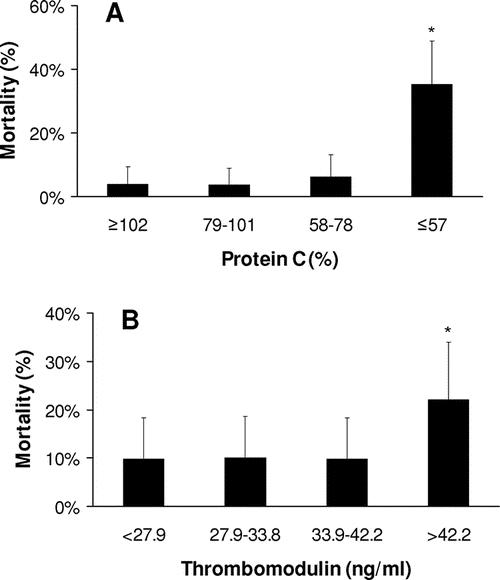
Results: A total of 208 patients were enrolled. Patients without tissue hypoperfusion were not coagulopathic, irrespective of the amount of thrombin generated. Prolongation of the partial thromboplastin and prothrombin times was only observed with an increased BD. An increasing BD was associated with high soluble thrombomodulin and low protein C levels. Low protein C levels were associated with prolongation of the partial thromboplastin and prothrombin times and hyperfibrinolysis with low levels of plasminogen activator inhibitor-1 and high D-dimer levels. High thrombomodulin and low protein C levels were significantly associated with increased mortality, blood transfusion requirements, acute renal injury, and reduced ventilator-free days.
Conclusions: Early traumatic coagulopathy occurs only in the presence of tissue hypoperfusion and appears to occur without significant consumption of coagulation factors. Alterations in the thrombomodulin-protein C pathway are consistent with activated protein C activation and systemic anticoagulation. Admission plasma thrombomodulin and protein C levels are predictive of clinical outcomes following major trauma.
Figures
References
-
- Mathers CD, Lopez A, Stein C, et al. Deaths and disease burden by cause: global burden of disease estimates for 2001 by World Bank country groups. Fogarty International Center, National Institutes of Health, 2003. Available at http://www.fic.nih.gov/dcpp/wps/wp18.pdf. Accessed December 16, 2005.
-
- Injury Chart Book. Geneva: World Health Organization; 2002. Available at http://www.who.int/violence_injury_prevention/injury/chartbook/chartb/en/. Accessed December 16, 2005.
-
- Armand R, Hess JR. Treating coagulopathy in trauma patients. Transfus Med Rev. 2003;17:223–231. - PubMed
-
- College of American Pathologists. Practice parameters for the use of fresh frozen plasma, cryoprecipitate and platelets. JAMA. 1994;271:777–781. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
