

Advanced imaging and visualization in gastrointestinal disorders
- PMID: 17457973
- PMCID: PMC4146926
- DOI: 10.3748/wjg.v13.i9.1408
Advanced imaging and visualization in gastrointestinal disorders
Abstract
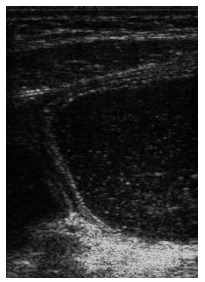
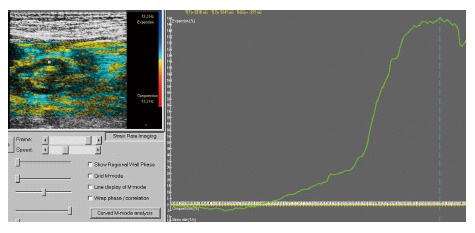
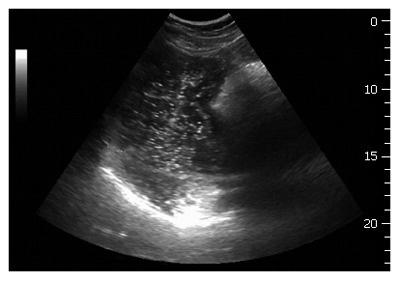
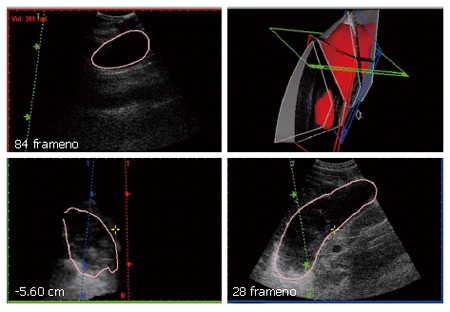
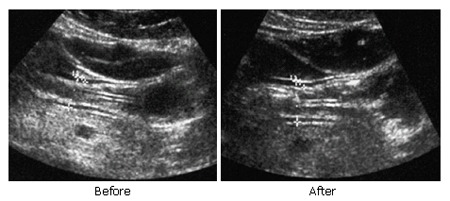
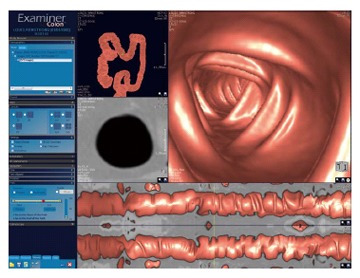
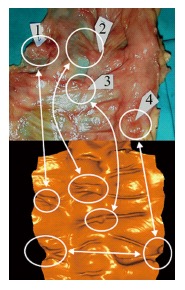
Advanced medical imaging and visualization has a strong impact on research and clinical decision making in gastroenterology. The aim of this paper is to show how imaging and visualization can disclose structural and functional abnormalities of the gastrointestinal (GI) tract. Imaging methods such as ultrasonography, magnetic resonance imaging (MRI), endoscopy, endosonography, and elastography will be outlined and visualization with Virtual Reality and haptic methods. Ultrasonography is a versatile method that can be used to evaluate antral contractility, gastric emptying, transpyloric flow, gastric configuration, intragastric distribution of meals, gastric accommodation and strain measurement of the gastric wall. Advanced methods for endoscopic ultrasound, three-dimensional (3D) ultrasound, and tissue Doppler (Strain Rate Imaging) provide detailed information of the GI tract. Food hypersensitivity reactions including gastrointestinal reactions due to food allergy can be visualized by ultrasonography and MRI. Development of multi-parametric and multi-modal imaging may increase diagnostic benefits and facilitate fusion of diagnostic and therapeutic imaging in the future.
Figures

References
-
- Gilja OH, Hausken T, Ødegaard S, Wendelbo Ø, Thierley M. Mobile ultrasonography in a medical department. Tidsskr Nor Laegeforen. 2003;123:2713–2714. - PubMed
-
- Bateman DN, Leeman S, Metreweli C, Willson K. A non-invasive technique for gastric motility measurement. Br J Radiol. 1977;50:526–527. - PubMed
-
- Hausken T, Berstad A. Wide gastric antrum in patients with non-ulcer dyspepsia. Effect of cisapride. Scand J Gastroenterol. 1992;27:427–432. - PubMed
-
- Hausken T, Odegaard S, Berstad A. Antroduodenal motility studied by real-time ultrasonography. Effect of enprostil. Gastroenterology. 1991;100:59–63. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
