

Concepts and preliminary data toward the realization of image-guided liver surgery
- PMID: 17458587
- PMCID: PMC3839065
- DOI: 10.1007/s11605-007-0090-6
Concepts and preliminary data toward the realization of image-guided liver surgery
Abstract
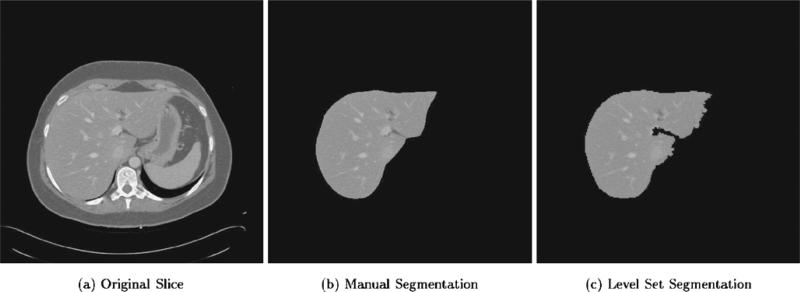
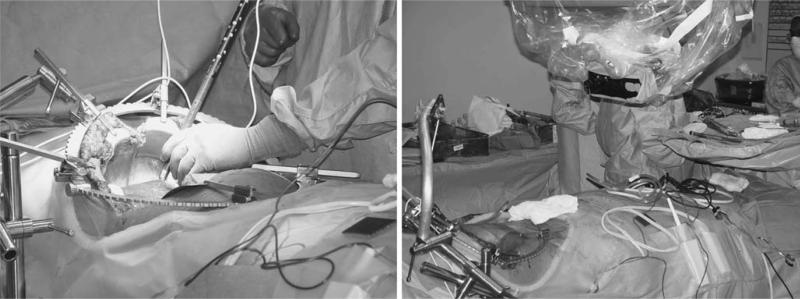
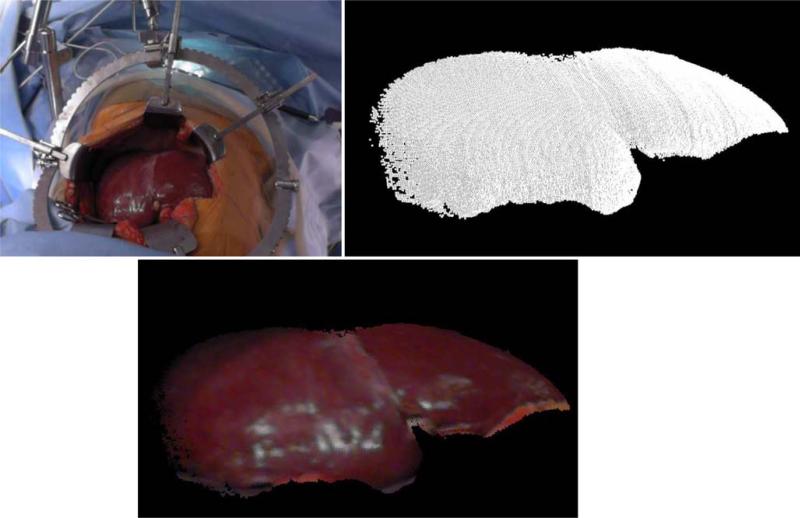
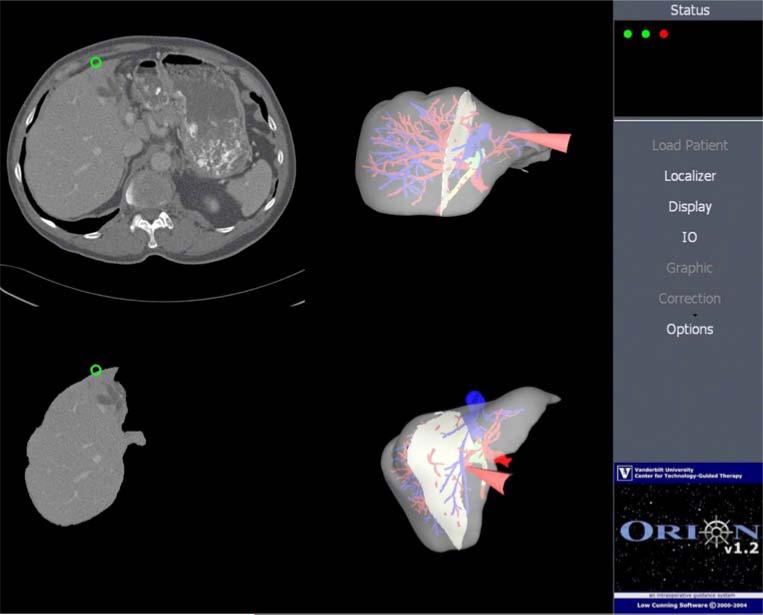
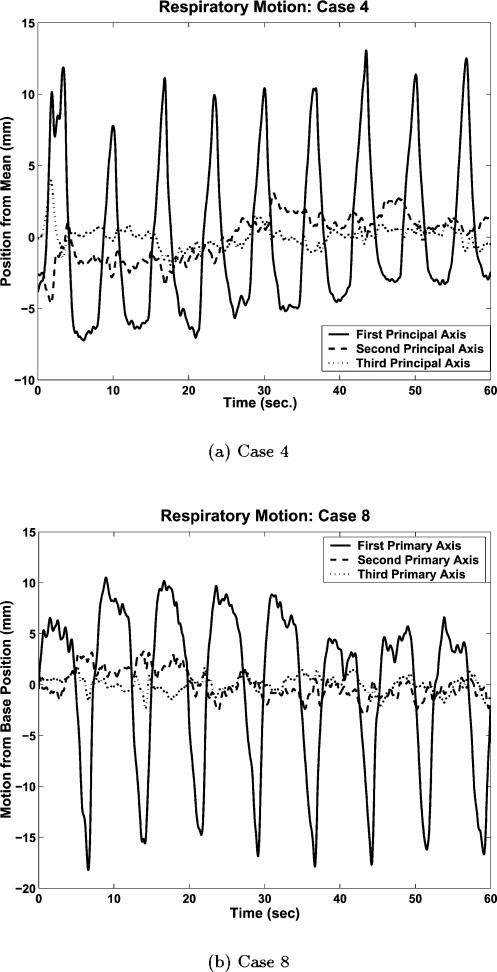
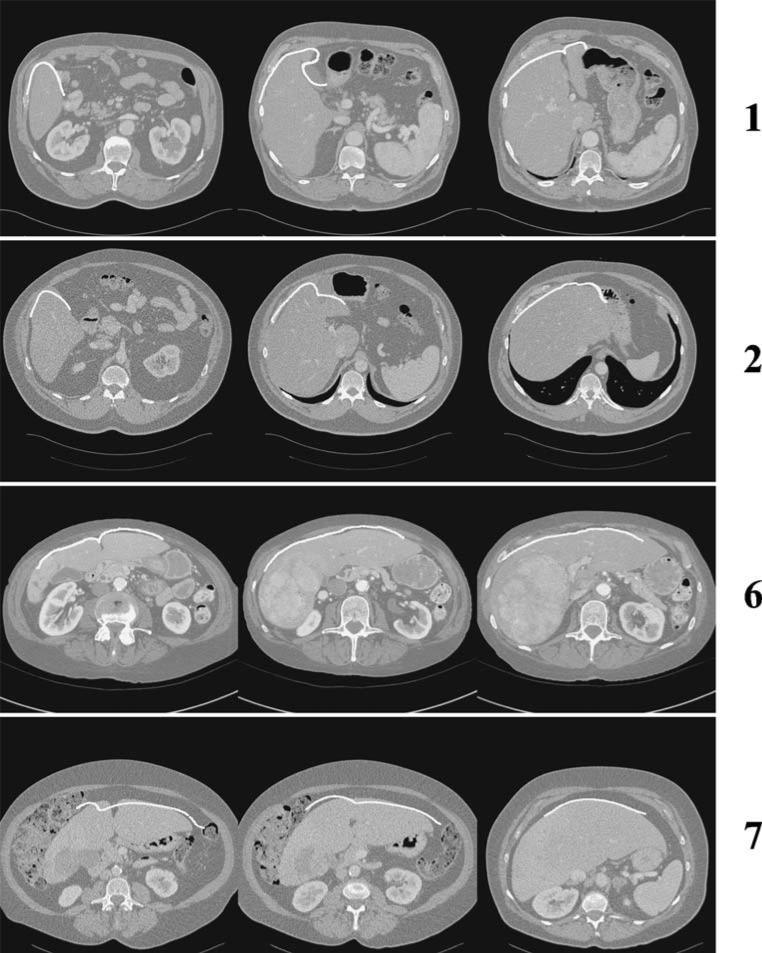
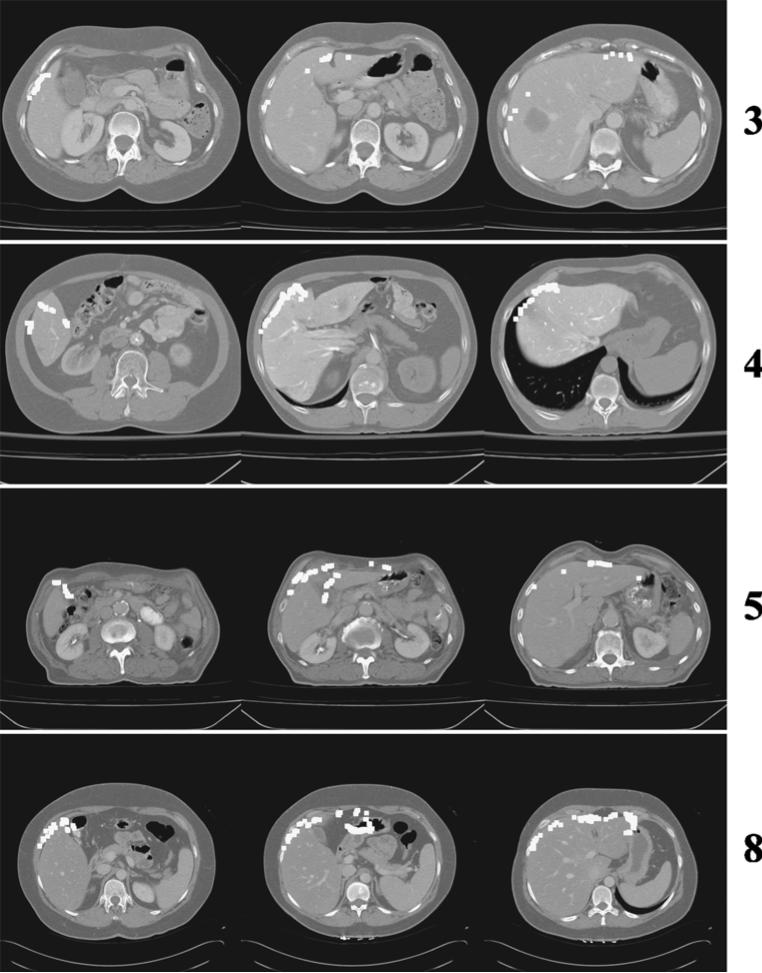
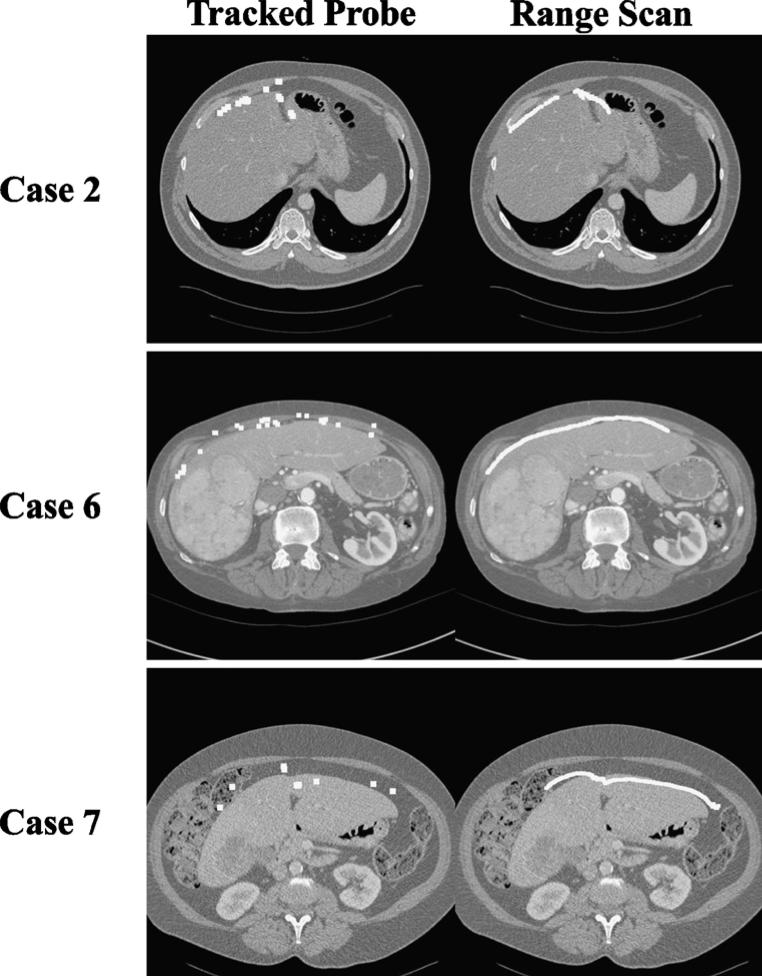
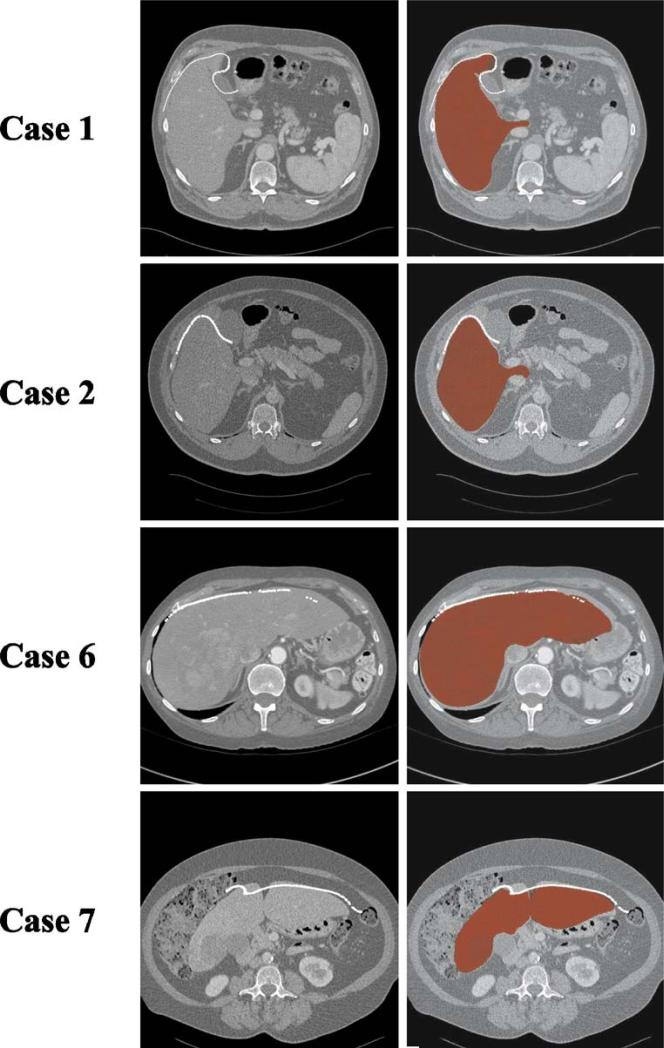
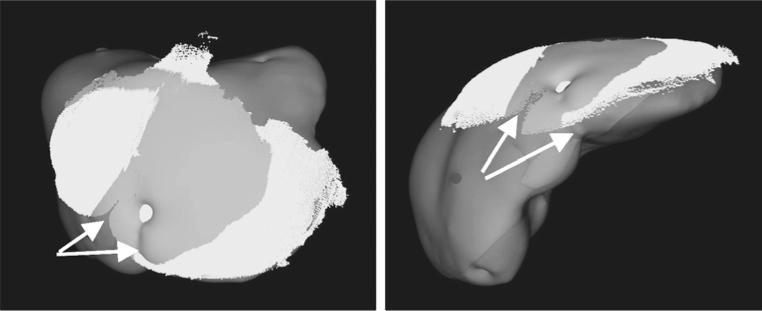
Image-guided surgery provides navigational assistance to the surgeon by displaying the surgical probe position on a set of preoperative tomograms in real time. In this study, the feasibility of implementing image-guided surgery concepts into liver surgery was examined during eight hepatic resection procedures. Preoperative tomographic image data were acquired and processed. Accompanying intraoperative data on liver shape and position were obtained through optically tracked probes and laser range scanning technology. The preoperative and intraoperative representations of the liver surface were aligned using the iterative closest point surface matching algorithm. Surface registrations resulted in mean residual errors from 2 to 6 mm, with errors of target surface regions being below a stated goal of 1 cm. Issues affecting registration accuracy include liver motion due to respiration, the quality of the intraoperative surface data, and intraoperative organ deformation. Respiratory motion was quantified during the procedures as cyclical, primarily along the cranial-caudal direction. The resulting registrations were more robust and accurate when using laser range scanning to rapidly acquire thousands of points on the liver surface and when capturing unique geometric regions on the liver surface, such as the inferior edge. Finally, finite element models recovered much of the observed intraoperative deformation, further decreasing errors in the registration. Image-guided liver surgery has shown the potential to provide surgeons with important navigation aids that could increase the accuracy of targeting lesions and the number of patients eligible for surgical resection.
Figures

References
-
- American Cancer Society . Cancer Facts And Figures. 2004. Available at http://www.cancer.org.
-
- Steele GD., Jr The national cancer data base report on colorectal cancer. Cancer. 1994;74:1979–1989. - PubMed
-
- Bengmark S, Hafstrom L. The natural history of primary and secondary malignant tumors of the liver. I. The prognosis for patients with hepatic metastases from colonic and rectal carcinoma by laparotomy. Cancer. 1969;23:198–202. - PubMed
-
- Wood CB, Gillis CR, Blumgart LH. A retrospective study of the natural history of patients with liver metastases from colorectal cancer. Clin Oncol. 1976;2:285–288. - PubMed
-
- Zavadsky KE, Lee YT. Liver metastases from colorectal– carcinoma—incidence, resectability, and survival results. Am Surg. 1994;60:929–933. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
