

Current surgical treatment for bile duct cancer
- PMID: 17461441
- PMCID: PMC4146891
- DOI: 10.3748/wjg.v13.i10.1505
Current surgical treatment for bile duct cancer
Abstract
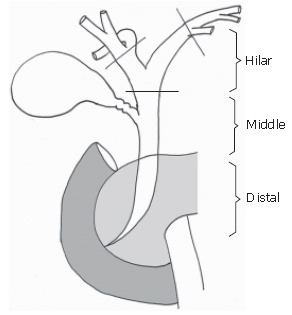
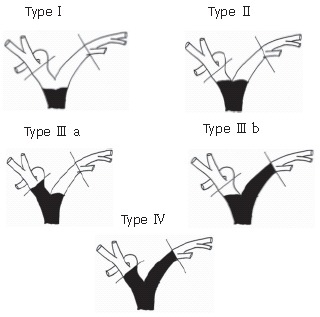
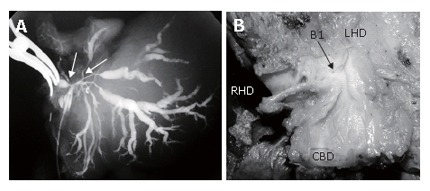
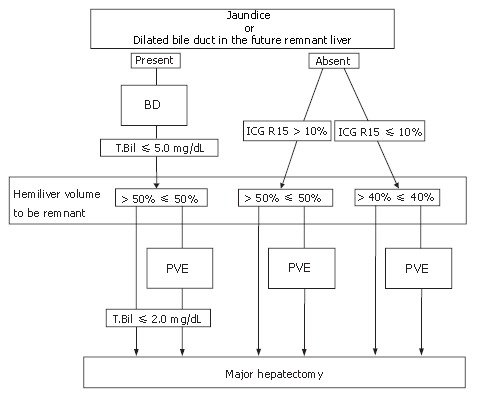
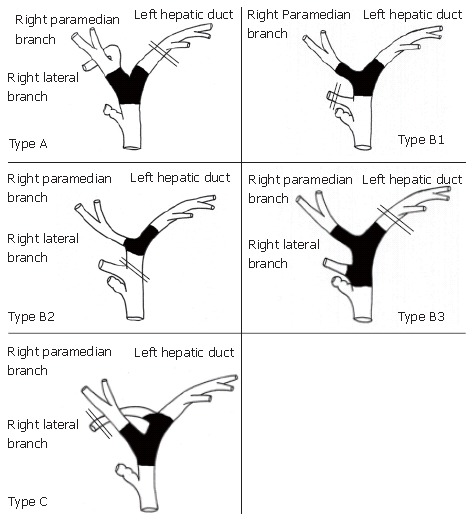
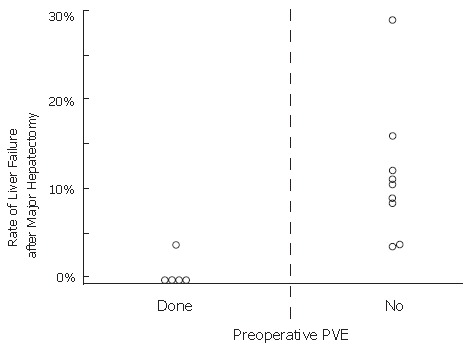
Since extrahepatic bile duct cancer is difficult to diagnose and to cure, a safe and radical surgical strategy is needed. In this review, the modes of infiltration and spread of extrahepatic bile duct cancer and surgical strategy are discussed. Extended hemihepatectomy, with or without pancreatoduodenectomy (PD), plus extrahepatic bile duct resection and regional lymphadenectomy has recently been recognized as the standard curative treatment for hilar bile duct cancer. On the other hand, PD is the choice of treatment for middle and distal bile duct cancer. Major hepatectomy concomitant with PD (hepatopancreatoduodenectomy) has been applied to selected patients with widespread tumors. Preoperative biliary drainage (BD) followed by portal vein embolization (PVE) enables major hepatectomy in patients with hilar bile duct cancer without mortality. BD should be performed considering the surgical procedure, especially, in patients with separated intrahepatic bile ducts caused by hilar bile duct cancer. Right or left trisectoriectomy are indicated according to the tumor spread and biliary anatomy. As a result, extended radical resection offers a chance for cure of hilar bile duct cancer with improved resectability, curability, and a 5-year survival rate of 40%. A 5-year survival rate has ranged from 24% to 39% after PD for middle and distal bile duct cancer.
Figures

References
-
- Klatskin G. Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis. An unusual tumor with distinctive clinical and pathological features. Am J Med. 1965;38:241–256. - PubMed
-
- Bismuth H, Corlette MB. Intrahepatic cholangioenteric anastomosis in carcinoma of the hilus of the liver. Surg Gynecol Obstet. 1975;140:170–178. - PubMed
-
- Blumgart LH, Hadjis NS, Benjamin IS, Beazley R. Surgical approaches to cholangiocarcinoma at confluence of hepatic ducts. Lancet. 1984;1:66–70. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
