

Clinical characteristics of idiopathic portal hypertension
- PMID: 17461489
- PMCID: PMC4146965
- DOI: 10.3748/wjg.v13.i13.1906
Clinical characteristics of idiopathic portal hypertension
Abstract
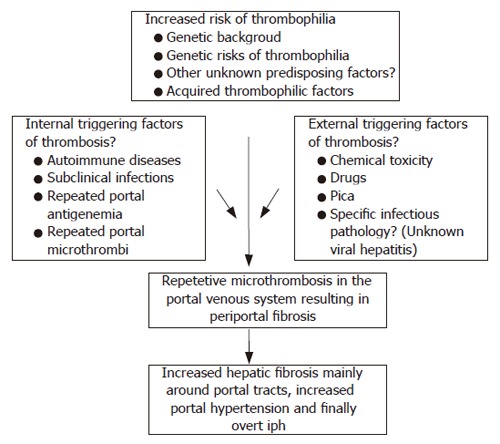
Idiopathic portal hypertension is one of the interesting causes of portal hypertension. Even in very developed medical centers, this disorder is still one of the most important misdiagnoses of clinical practice. To inexperienced physicians, presenting esophageal varices and upper gastrointestinal bleeding usually prompt an unfortunate diagnosis of cirrhosis. A heterogenous clinical presentation and progression of this disorder should be recognized by physicians, and management should be directed towards some specific problems confined to this disorder. Although a genetic basis and other factors are implicated in its pathogenesis, exact underlying mechanism(s) is (are) unknown. In this review, we discuss the heterogeneity of idiopathic portal hypertension, its etiopathogenesis, clinical presentation and management issues. With the expectation of an excellent prognosis, a practicing gastroenterologist should be aware that "not all varices mean cirrhosis".
Figures


Similar articles
-
[Controversies in therapy of portal hypertension and bleeding esophageal varices].Internist (Berl). 1994 Apr;35(4):355-62. Internist (Berl). 1994. PMID: 8200760 Review. German. No abstract available.
-
The management of portal hypertension: controversies.J Gastroenterol Hepatol. 2002 Dec;17 Suppl:S439-40. doi: 10.1046/j.1440-1746.17.s4.6.x. J Gastroenterol Hepatol. 2002. PMID: 12534774 Review. No abstract available.
-
Advances in the treatment of portal hypertension in cirrhosis.Expert Rev Gastroenterol Hepatol. 2016 Aug;10(8):961-9. doi: 10.1586/17474124.2016.1166952. Epub 2016 Mar 28. Expert Rev Gastroenterol Hepatol. 2016. PMID: 26982499 Review.
-
Portal hypertension and varices in patients with liver cirrhosis.Nurs Stand. 2012 Aug 1-7;26(48):52-7; quiz 58. doi: 10.7748/ns2012.08.26.48.52.c9230. Nurs Stand. 2012. PMID: 22916658
-
Bleeding esophageal varices. How to treat this dreaded complication of portal hypertension.Postgrad Med. 2001 Feb;109(2):75-6, 81-6, 89. doi: 10.3810/pgm.2001.02.852. Postgrad Med. 2001. PMID: 11272695 Review.
Cited by
-
Spleen stiffness measurements using point shear wave elastography detects noncirrhotic portal hypertension in human immunodeficiency virus.Medicine (Baltimore). 2019 Nov;98(47):e17961. doi: 10.1097/MD.0000000000017961. Medicine (Baltimore). 2019. PMID: 31764798 Free PMC article.
-
Analysis of inherited thrombophilic mutations and natural anticoagulant deficiency in patients with idiopathic portal hypertension.J Thromb Thrombolysis. 2009 Jul;28(1):57-62. doi: 10.1007/s11239-008-0244-8. Epub 2008 Aug 7. J Thromb Thrombolysis. 2009. PMID: 18685811
-
Outcomes of partial splenic embolization in patients with massive splenomegaly due to idiopathic portal hypertension.World J Gastroenterol. 2016 Nov 21;22(43):9623-9630. doi: 10.3748/wjg.v22.i43.9623. World J Gastroenterol. 2016. PMID: 27920483 Free PMC article.
-
Celiac disease as a potential cause of idiopathic portal hypertension: a case report.J Med Case Rep. 2009 Feb 16;3:68. doi: 10.1186/1752-1947-3-68. J Med Case Rep. 2009. PMID: 19220902 Free PMC article.
-
Idiopathic portal hypertension in an "inactive" HBV carrier: a case report.Cases J. 2008 Oct 8;1(1):229. doi: 10.1186/1757-1626-1-229. Cases J. 2008. PMID: 18842148 Free PMC article.
References
-
- Sarin SK, Aggarwal SR. Idiopathic portal hypertension. Digestion. 1998;59:420–423. - PubMed
-
- Huet PM, Guillaume E, Cote J, Légaré A, Lavoie P, Viallet A. Noncirrhotic presinusoidal portal hypertension associated with chronic arsenical intoxication. Gastroenterology. 1975;68:1270–1277. - PubMed
-
- Thomas LB, Popper H, Berk PD, Selikoff I, Falk H. Vinyl-chloride-induced liver disease. From idiopathic portal hypertension (Banti's syndrome) to Angiosarcomas. N Engl J Med. 1975;292:17–22. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
