

Hepatic venous outflow obstruction: three similar syndromes
- PMID: 17461490
- PMCID: PMC4146966
- DOI: 10.3748/wjg.v13.i13.1912
Hepatic venous outflow obstruction: three similar syndromes
Abstract
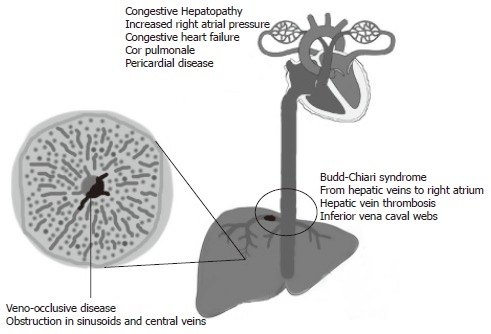
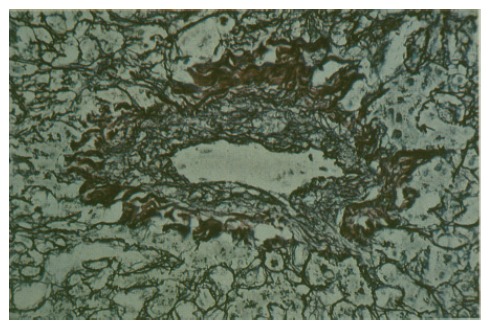
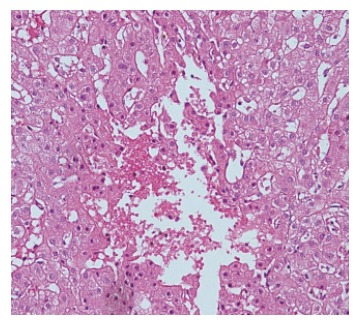
Our goal is to provide a detailed review of veno-occlusive disease (VOD), Budd-Chiari syndrome (BCS), and congestive hepatopathy (CH), all of which results in hepatic venous outflow obstruction. This is the first article in which all three syndromes have been reviewed, enabling the reader to compare the characteristics of these disorders. The histological findings in VOD, BCS, and CH are almost identical: sinusoidal congestion and cell necrosis mostly in perivenular areas of hepatic acini which eventually leads to bridging fibrosis between adjacent central veins. Tender hepatomegaly with jaundice and ascites is common to all three conditions. However, the clinical presentation depends mostly on the extent and rapidity of the outflow obstruction. Although the etiology and treatment are completely different in VOD, BCS, and CH; the similarities in clinical manifestations and liver histology may suggest a common mechanism of hepatic injury and adaptation in response to increased sinusoidal pressure.
Figures
Similar articles
-
A comparative histopathological study of hepatic venous outflow obstruction in veno-occlusive disease and Budd-Chiari's syndrome.Changgeng Yi Xue Za Zhi. 1990 Sep;13(3):167-81. Changgeng Yi Xue Za Zhi. 1990. PMID: 2253098
-
The Spectrum of Histologic Findings in Hepatic Outflow Obstruction.Arch Pathol Lab Med. 2017 Jan;141(1):98-103. doi: 10.5858/arpa.2015-0388-OA. Epub 2016 Sep 28. Arch Pathol Lab Med. 2017. PMID: 27681331 Free PMC article.
-
Classification of hepatic venous outflow obstruction: ambiguous terminology of the Budd-Chiari syndrome.Mayo Clin Proc. 1990 Jan;65(1):51-5. doi: 10.1016/s0025-6196(12)62109-0. Mayo Clin Proc. 1990. PMID: 2296212
-
Primary Budd-Chiari syndrome versus sinusoidal obstruction syndrome: a review.Curr Med Res Opin. 2024 Feb;40(2):303-313. doi: 10.1080/03007995.2023.2288909. Epub 2024 Jan 24. Curr Med Res Opin. 2024. PMID: 38006404 Review.
-
[Veno-occlusive disease of the liver].Wiad Lek. 2009;62(1):42-51. Wiad Lek. 2009. PMID: 19817257 Review. Polish.
Cited by
-
Paediatric liver ultrasound: a pictorial essay.J Ultrasound. 2020 Mar;23(1):87-103. doi: 10.1007/s40477-018-0352-z. Epub 2019 Feb 18. J Ultrasound. 2020. PMID: 30778891 Free PMC article. Review.
-
Diagnostic performance of Contrast-enhanced CT in Pyrrolizidine Alkaloids-induced Hepatic Sinusoidal Obstructive Syndrome.Sci Rep. 2016 Nov 29;6:37998. doi: 10.1038/srep37998. Sci Rep. 2016. PMID: 27897243 Free PMC article.
-
Prognostic factors for pyrrolizidine alkaloid-induced hepatic sinusoidal obstruction syndrome: a multicenter study in China.Ann Transl Med. 2021 Jan;9(1):11. doi: 10.21037/atm-20-731. Ann Transl Med. 2021. PMID: 33553304 Free PMC article.
-
Hepatic veno-occlusive disease: a chemotherapy-related toxicity in children with malignancies.Paediatr Drugs. 2010 Oct 1;12(5):277-84. doi: 10.2165/11531840-000000000-00000. Paediatr Drugs. 2010. PMID: 20799757 Review.
-
The value of hepatic diffusion-weighted MR imaging in demonstrating hepatic congestion secondary to pulmonary hypertension.Cardiovasc Ultrasound. 2010 Jul 21;8:28. doi: 10.1186/1476-7120-8-28. Cardiovasc Ultrasound. 2010. PMID: 20663149 Free PMC article.
References
-
- Lautt WW, Greenway CV. Conceptual review of the hepatic vascular bed. Hepatology. 1987;7:952–963. - PubMed
-
- Rosenberg PM, Friedman LS. The liver in circulatory failure. In: Schiff ER, Sorrell MF, Maddrey WC, editors. Schiff's diseases of the liver. 9th ed. Philadelphia: Lippincott Williams & Wilkins; 2004. pp. 1327–1340.
-
- Shulman HM, McDonald GB, Matthews D, Doney KC, Kopecky KJ, Gauvreau JM, Thomas ED. An analysis of hepatic venocclusive disease and centrilobular hepatic degeneration following bone marrow transplantation. Gastroenterology. 1980;79:1178–1191. - PubMed
-
- Tanaka M, Wanless IR. Pathology of the liver in Budd-Chiari syndrome: portal vein thrombosis and the histogenesis of veno-centric cirrhosis, veno-portal cirrhosis, and large regenerative nodules. Hepatology. 1998;27:488–496. - PubMed
-
- Arora A, Tandon N, Sharma MP, Acharya SK. Constrictive pericarditis masquerading as Budd-Chiari syndrome. J Clin Gastroenterol. 1991;13:178–181. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
