

Recommendations on chronic constipation (including constipation associated with irritable bowel syndrome) treatment
- PMID: 17464377
- PMCID: PMC2794454
Recommendations on chronic constipation (including constipation associated with irritable bowel syndrome) treatment
Abstract
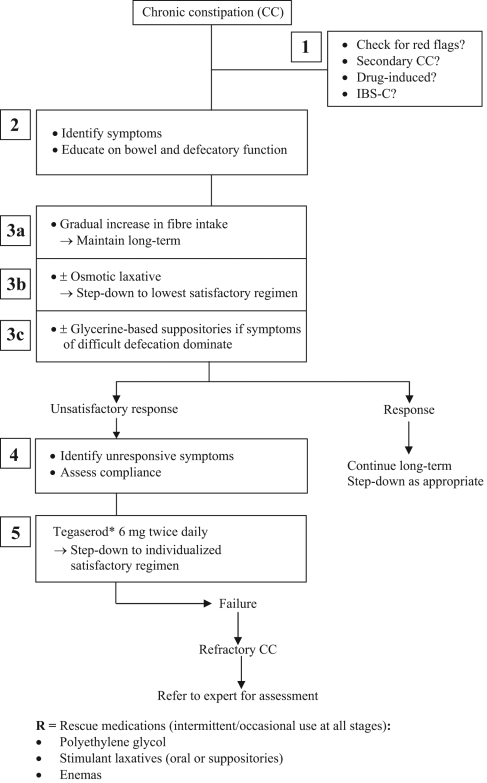
While chronic constipation (CC) has a high prevalence in primary care, there are no existing treatment recommendations to guide health care professionals. To address this, a consensus group of 10 gastroenterologists was formed to develop treatment recommendations. Although constipation may occur as a result of organic disease, the present paper addresses only the management of primary CC or constipation associated with irritable bowel syndrome. The final consensus group was assembled and the recommendations were created following the exact process outlined by the Canadian Association of Gastroenterology for the following areas: epidemiology, quality of life and threshold for treatment; definitions and diagnostic criteria; lifestyle changes; bulking agents and stool softeners; osmotic agents; prokinetics; stimulant laxatives; suppositories; enemas; other drugs; biofeedback and behavioural approaches; surgery; and probiotics. A treatment algorithm was developed by the group for CC and constipation associated with irritable bowel syndrome. Where possible, an evidence-based approach and expert opinions were used to develop the statements in areas with insufficient evidence. The nature of the underlying pathophysiology for constipation is often unclear, and it can be tricky for physicians to decide on an appropriate treatment strategy for the individual patient. The myriad of treatment options available to Canadian physicians can be confusing; thus, the main aim of the recommendations and treatment algorithm is to optimize the approach in clinical care based on available evidence.
La prévalence de la constipation chronique (CC) est élevée en soins primaires, mais il n’existe pas de recommandations de traitement pour orienter les professionnels de la santé. Pour régler cette lacune, on a formé un groupe consensuel de 10 gastroentérologues afin d’élaborer des recommandations de traitement. Certains cas de constipation découlent d’une maladie organique, mais le présent article ne porte que sur la prise en charge de la CC primaire ou sur la constipation reliée au syndrome du côlon irritable. On a créé le groupe consensuel final et établi les recommandations d’après le processus exact de l’Association canadienne de gastroentérologie dans les domaines suivants : épidémiologie, qualité de vie et seuil de traitement, définitions et critères diagnostiques, modifications au mode de vie, agents gonflants et laxatifs émollients, agents osmotiques, procinétiques, laxatifs stimulants, suppositoires, lavements, autres médicaments, rétroaction biologique (biofeedback) et approches behaviorales, chirurgie et probiotiques. Le groupe a conçu un algorithme de traitement de la CC et de la constipation associée au syndrome du côlon irritable. Dans la mesure du possible, elle a privilégié des démarches probantes et des avis d’experts pour élaborer des énoncés dans les domaines où les données étaient insuffisantes. Souvent, on ne connaît pas vraiment la nature de la physiopathologie sous-jacente à la constipation, et il peut être délicat pour les médecins de choisir une stratégie de traitement pertinente pour un patient donné. La myriade de possibilités de traitement offerte aux médecins canadiens peut susciter la confusion. Les recommandations et l’algorithme de traitement visent donc à optimiser la démarche de soins cliniques d’après les données disponibles.
Figures
References
-
- Nyam DC, Pemberton JH, Ilstrup DM, Rath DM. Long-term results of surgery for chronic constipation. Dis Colon Rectum. 1997;40:273–9. - PubMed
-
- Gonlachanvit S, Patcharatrakul T. Causes of idiopathic constipation in Thai patients: Associations between the causes and constipation symptoms as defined in the Rome II criteria. J Med Assoc Thai. 2004;87(Suppl 2):S22–8. - PubMed
-
- Prather CM. Subtypes of constipation: Sorting out the confusion. Rev Gastroenterol Disord. 2004;4(Suppl 2):S11–6. - PubMed
-
- Herve S, Savoye G, Behbahani A, Leroi AM, Denis P, Ducrotte P. Results of 24-h manometric recording of colonic motor activity with endoluminal instillation of bisacodyl in patients with severe chronic slow transit constipation. Neurogastroenterol Motil. 2004;16:397–402. - PubMed
-
- Rao SS, Sadeghi P, Beaty J, Kavlock R. Ambulatory 24-hour colonic manometry in slow-transit constipation. Am J Gastroenterol. 2004;99:2405–16. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical