

Preoperative diagnosis of gastrointestinal stromal tumor by endoscopic ultrasound-guided fine needle aspiration
- PMID: 17465451
- PMCID: PMC4319128
- DOI: 10.3748/wjg.v13.i14.2077
Preoperative diagnosis of gastrointestinal stromal tumor by endoscopic ultrasound-guided fine needle aspiration
Abstract
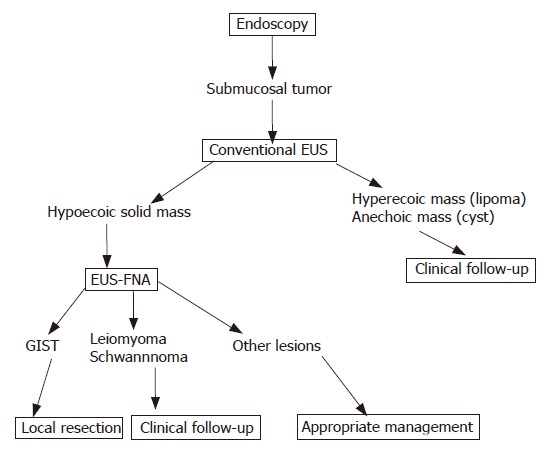
Aim: To evaluate the role of endoscopic ultrasonography-guided fine needle aspiration (EUS-FNA) in the preoperative diagnosis of gastrointestinal stromal tumor (GIST).
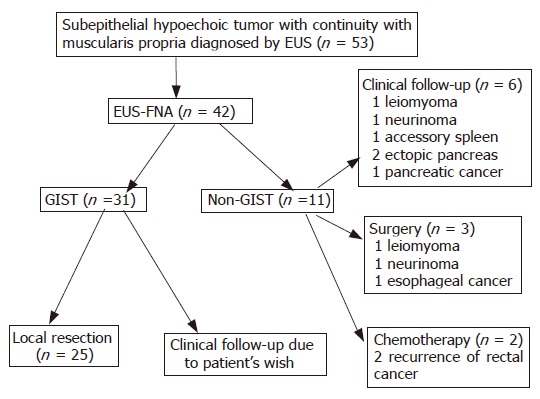
Methods: From September 2002 to June 2006, Fifty-three consecutive EUS-FNAs of GI tract subepithelial hypoechoic tumors with continuity to proper muscle layer suspected as GIST by standard EUS were evaluated prospectively. The reference standards for the final diagnosis were surgery (n = 31), or clinical follow-up (n=22). Additionally, immunophenotyping of specimens obtained by EUS-FNA and surgical resection specimens were compared.
Results: In 2 cases puncture was not performed because of anatomical problems. The collection rate of adequate specimens from the GI tract subepithelial hypoechoic tumor with continuity to proper muscle layer was 82% (42/51). The diagnostic rate for the tumor less than 2 cm, 2 to 4 cm, and 4 cm or more were 71% (15/21), 86% (18/21), and 100% (9/9), respectively. In 29 surgically resected cases, the sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic accuracy of EUS-FNA using immunohistochemical analysis of GIST were 100% (24/24), 80% (4/5), 96% (24/25), 100% (4/4), and 97% (28/29), respectively. No major complications were encountered.
Conclusion: EUS-FNA with immunohistochemical analysis is a safe and accurate method in the pretherapeutic diagnosis of GIST. It should be taken into consideration in decision making, especially in early diagnosis following minimal invasive surgery for GIST.
Figures

References
-
- Blay JY, Bonvalot S, Casali P, Choi H, Debiec-Richter M, Dei Tos AP, Emile JF, Gronchi A, Hogendoorn PC, Joensuu H, et al. Consensus meeting for the management of gastrointestinal stromal tumors. Report of the GIST Consensus Conference of 20-21 March 2004, under the auspices of ESMO. Ann Oncol. 2005;16:566–578. - PubMed
-
- Miettinen M, Sarlomo-Rikala M, Lasota J. Gastrointestinal stromal tumors: recent advances in understanding of their biology. Hum Pathol. 1999;30:1213–1220. - PubMed
-
- Nishida T, Hirota S. Biological and clinical review of stromal tumors in the gastrointestinal tract. Histol Histopathol. 2000;15:1293–1301. - PubMed
-
- Rubin BP, Fletcher JA, Fletcher CD. Molecular Insights into the Histogenesis and Pathogenesis of Gastrointestinal Stromal Tumors. Int J Surg Pathol. 2000;8:5–10. - PubMed
-
- Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, Miettinen M, O'Leary TJ, Remotti H, Rubin BP, et al. Diagnosis of gastrointestinal stromal tumors: A consensus approach. Hum Pathol. 2002;33:459–465. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
