

Clinical results with the Trabectome, a novel surgical device for treatment of open-angle glaucoma
- PMID: 17471324
- PMCID: PMC1809927
Clinical results with the Trabectome, a novel surgical device for treatment of open-angle glaucoma
Abstract
Purpose: To describe treatment outcomes after Trabectome surgery in an initial series of 101 patients with open-angle glaucoma.
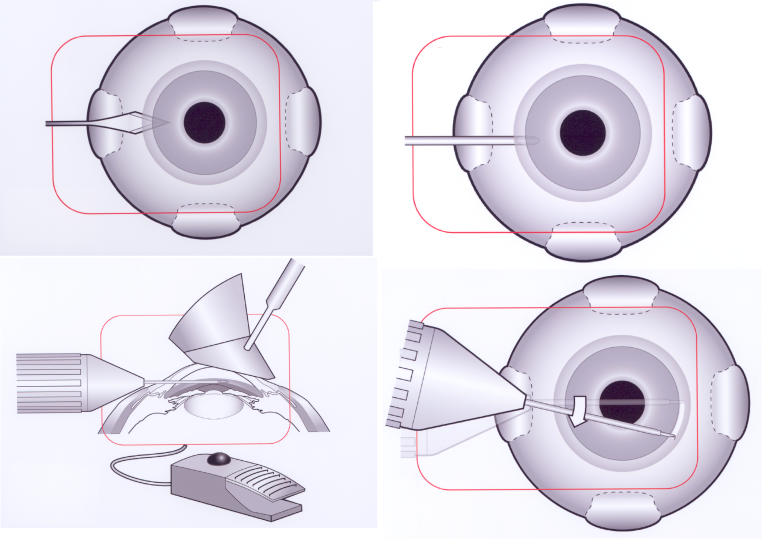
Methods: A 19-gauge microelectrosurgical device enabled ab interno removal of a strip of trabecular meshwork and inner wall of Schlemm's canal under gonioscopic control with continual infusion and foot-pedal control of aspiration and electrosurgery. A smooth, pointed ceramic-coated insulating footplate was inserted into Schlemm's canal to act as a guide within the canal and to protect adjacent structures from mechanical or heat injury during ablation of a 30- to 90-degree arc of angle tissue.
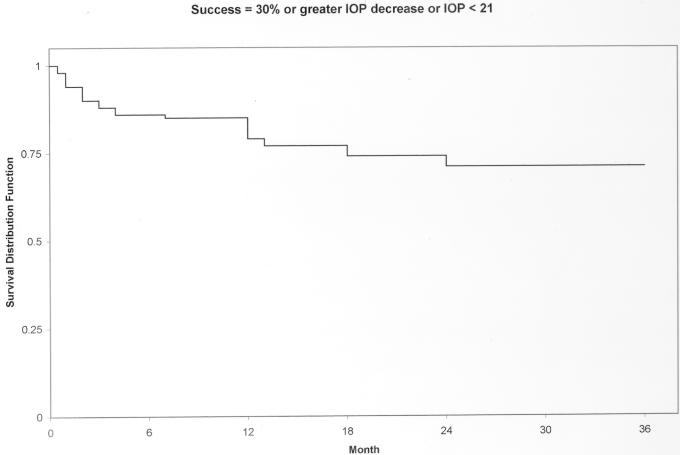
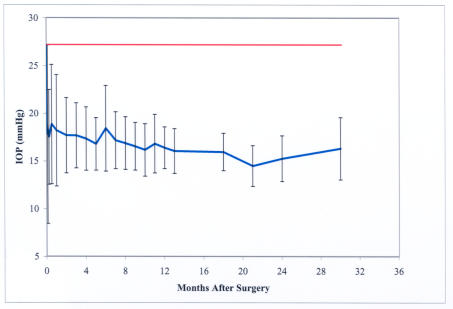
Results: Mean preoperative intraocular pressure (IOP) in the initial 101 patients was 27.6 +/- 7.2 mm Hg. Thirty months postoperatively, mean IOP was 16.3 +/- 3.3 mm Hg (n = 11). The mean percentage drop over the whole course of follow-up was 40%. At all times postoperatively, the absolute and percent decrease in IOP from preoperative levels were statistically significant (paired t test, P < .0001). Overall success (IOP </= 21 mm Hg with or without medications and no subsequent surgery) was 84%. Nine eyes subsequently underwent trabeculectomy, two others had IOP greater than 21 mm Hg in spite of resuming topical medications, and the rest of the patients either refused to resume medications or were still in the 1-month postoperative period without medications (total failure rate including trabeculectomies, 16/101 = 16%). Intraoperative reflux bleeding occurred in 100% of cases. Complications have been minimal and not vision-threatening.
Conclusions: The Trabectome facilitates minimally invasive and effective glaucoma surgery, which spares the conjunctiva and does not preclude subsequent standard filtering procedures.
Figures

References
-
- Chinhara E, Nishida A, Kodo M, Yoshimura N, Matsumura M, Yamamoto M, Takako T. Trabeculotomy ab externo: an alternative treatment in adult patients with primary open-angle glaucoma. Ophthalmic Surg. 1993;24:735–739. - PubMed
-
- Tanihara H, Negi A, Akimoto M, Nagata M. Long-term surgical results of combined trabeculotomy ab externo and cataract extraction. Ophthalmic Surg. 1995;26:316–324. - PubMed
-
- Tanihara H, Negi A, Akimoto M, Terauchi H, Okudaira A, Kozaki J, Takeuchi A, Nagata M. Surgical effects of trabeculotomy ab externo on adult eyes with primary open-angle glaucoma and pseudoexfoliation syndrome. Arch Ophthalmol. 1993;111:1653–1661. - PubMed
-
- Gimbel HV, Meyer D. Small incision trabeculotomy combined with phacoemulsification and intraocular lens implantation. JCRS. 1993;19:92–96. - PubMed
-
- Quaranta L, Hitchings RA, Quaranta CA. Ab-Interno goniotrabeculotomy versus mitomycin C trabeculectomy for adult open-angle glaucoma. Ophthalmology. 1999;106:1357–1362. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
