

A patient with encephalitis associated with NMDA receptor antibodies
- PMID: 17479076
- PMCID: PMC1936221
- DOI: 10.1038/ncpneuro0493
A patient with encephalitis associated with NMDA receptor antibodies
Abstract
Background: A 34-year-old woman presented with headache, feverish sensation and anxiety, rapidly followed by homicidal ideation, aggressive agitation, seizures, hypoventilation, hyperthermia and prominent autonomic instability requiring intubation and sedation. She developed episodes of hypotension and bradycardia with periods of asystole lasting up to 15 seconds. Upon weaning off sedation, her eyes opened but she was unresponsive to stimuli. There was muscle rigidity, frequent facial grimacing, rhythmic abdominal contractions, kicking motions of the legs, and intermittent dystonic postures of the right arm.
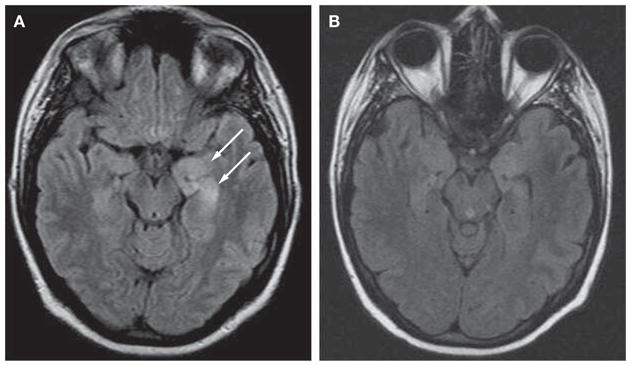
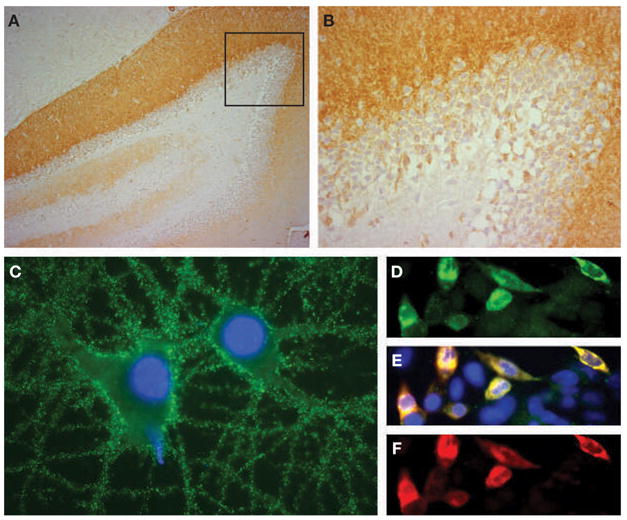
Investigations: Routine laboratory testing, toxicology screening, studies for autoimmune and infectious etiologies, brain MRI scan, lumbar puncture, electroencephalogram, whole-body CT scan, abdominal ultrasound, paraneoplastic and voltage-gated potassium channel antibody serologies, analysis of N-methyl-D-aspartate receptor antibodies.
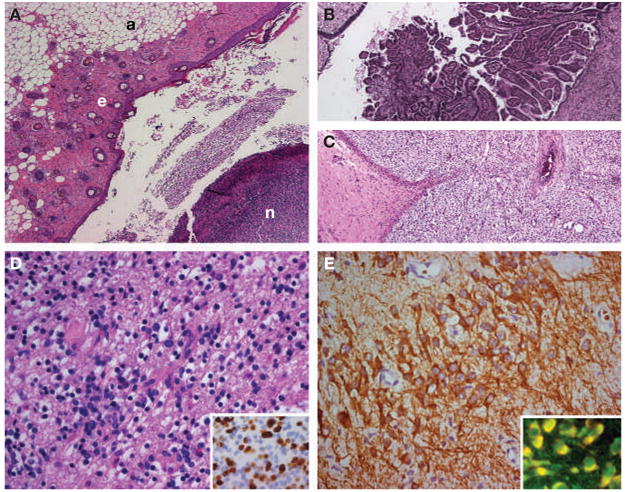
Diagnosis: Paraneoplastic encephalitis associated with immature teratoma of the ovary and N-methyl-D-aspartate receptor antibodies.
Management: Intensive care, mechanical ventilation, antiepileptics, laparotomy and left salpingo-oophorectomy, corticosteroids, plasma exchange, intravenous immunoglobulin, cyclophosphamide, physical therapy, and chemotherapy.
Figures
References
-
- Stein-Wexler R, et al. Paraneoplastic limbic encephalitis in a teenage girl with an immature ovarian teratoma. Pediatr Radiol. 2005;35:694–697. - PubMed
-
- Koide R, et al. EFA6A-like antibodies in paraneoplastic encephalitis associated with immature ovarian teratoma: a case report. J Neurooncol. 2007;81:71–74. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical