

Left ventricular form and function revisited: applied translational science to cardiovascular ultrasound imaging
- PMID: 17485001
- PMCID: PMC1951787
- DOI: 10.1016/j.echo.2006.10.013
Left ventricular form and function revisited: applied translational science to cardiovascular ultrasound imaging
Abstract
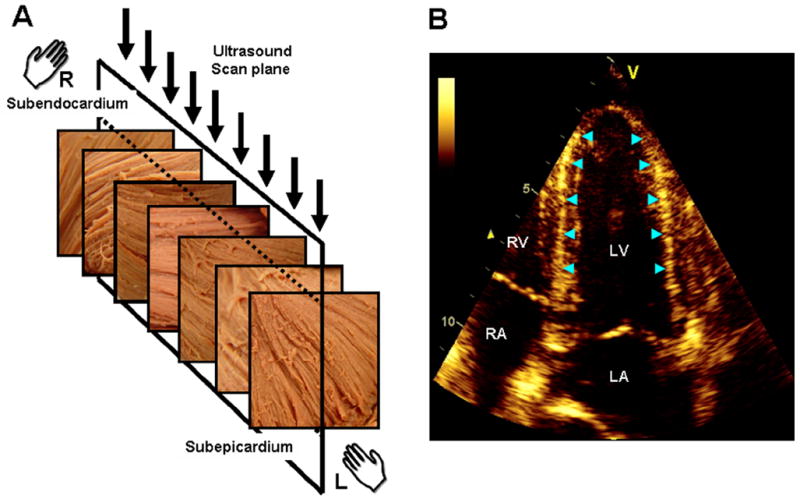
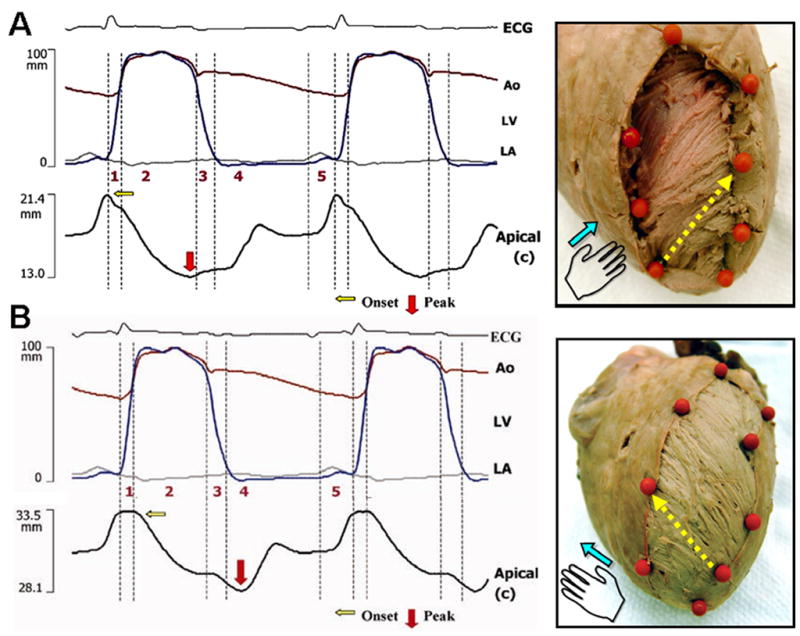
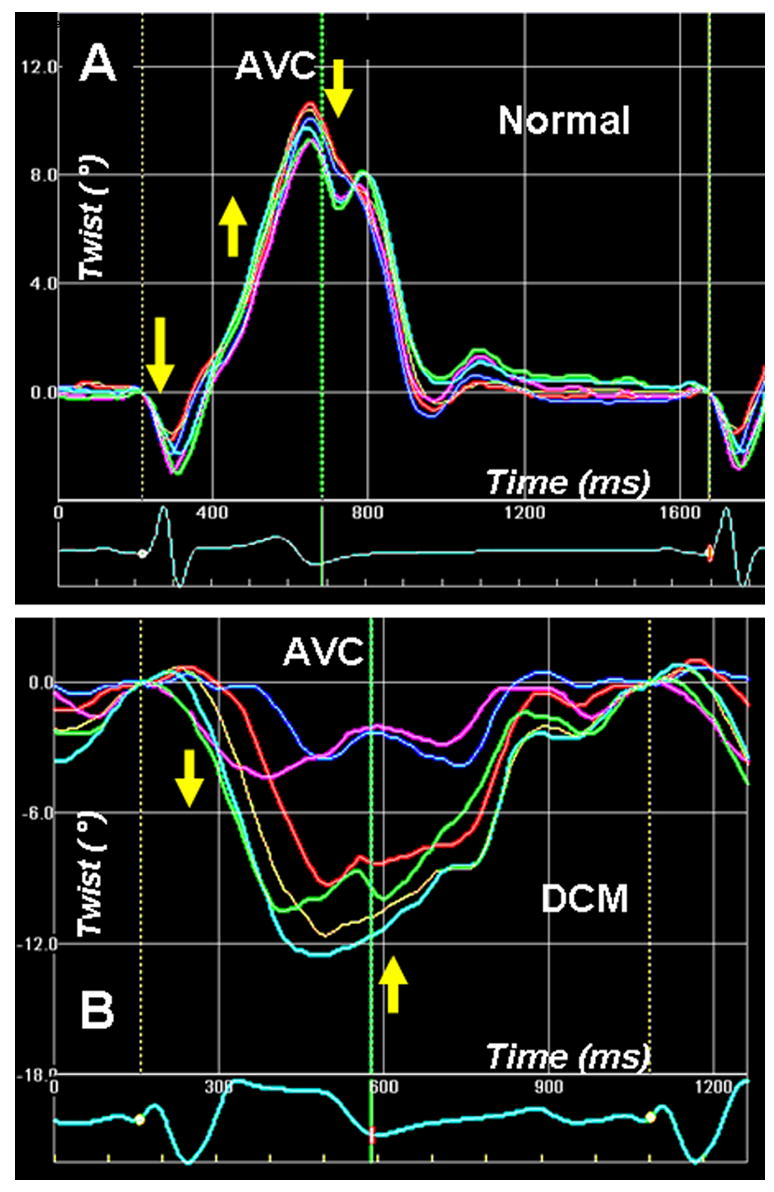
Doppler tissue imaging (DTI) and DTI-derived strain imaging are robust physiologic tools used for the noninvasive assessment of regional myocardial function. As a result of high temporal and spatial resolution, regional function can be assessed for each phase of the cardiac cycle and within the transmural layers of the myocardial wall. Newer techniques that measure myocardial motion by speckle tracking in gray-scale images have overcome the angle dependence of DTI strain, allowing for measurement of 2-dimensional strain and cardiac rotation. DTI, DTI strain, and speckle tracking may provide unique information that deciphers the deformation sequence of complexly oriented myofibers in the left ventricular wall. The data are, however, limited. This review examines the structure and function of the left ventricle relative to the potential clinical application of DTI and speckle tracking in assessing the global mechanical sequence of the left ventricle in vivo.
Figures
References
-
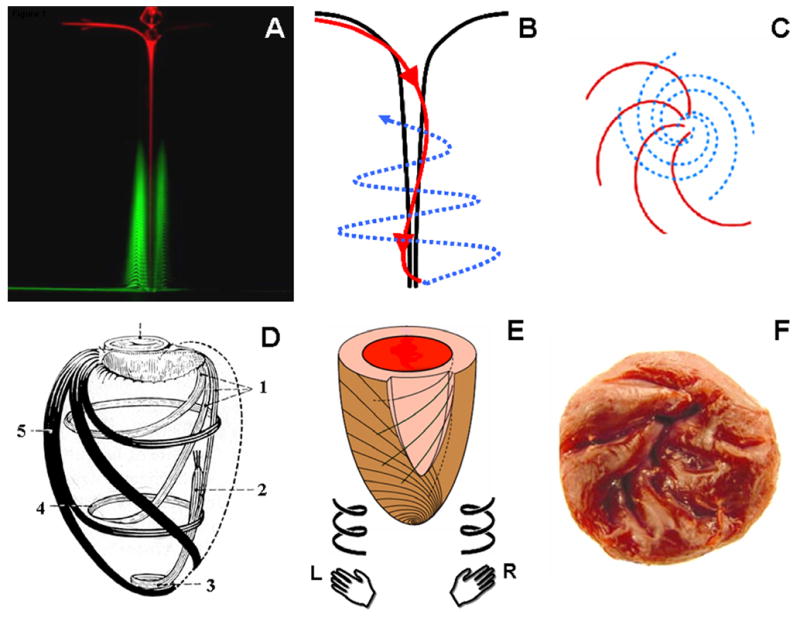
- Klar AJ. Fibonacci’s flowers. Nature. 2002;417:595. - PubMed
-
- Wurman J, Straka JM, Rasmussen EN. Fine-Scale Doppler Radar Observations of Tornadoes. Science. 1996;272:1774–7. - PubMed
-
- Lin CC. Global spiral patterns in galaxies: complexity and simplicity. Ann N Y Acad Sci. 1998;867:229–52. - PubMed
-
- Andersen A, Bohr T, Stenum B, Rasmussen JJ, Lautrup B. Anatomy of a bathtub vortex. Phys Rev Lett. 2003;91:104502. - PubMed
-
- Holdrege C. The Heart: A Pulsing and Perceptive Center. In: Holdrege C, editor. The Dynamic Heart and Circulation. Fair Oaks, CA: AWSNA Publications; 2002. p. 8.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
