

Review
doi: 10.1102/1470-7330.2007.0008.
Imaging of salivary gland tumours
Affiliations
- PMID: 17485257
- PMCID: PMC1866314
- DOI: 10.1102/1470-7330.2007.0008
Item in Clipboard
Review
Imaging of salivary gland tumours
Cancer Imaging.
.
Abstract
Imaging of salivary gland tumours is a major challenge for radiologists due to the great variety of differential diagnoses. This article gives a short overview on the anatomy of the salivary glands, the epidemiology of salivary gland tumours as well as the clinical presentation and the different imaging modalities including new magnetic resonance techniques such as diffusion-weighted magnetic resonance imaging, dynamic contrast-enhanced magnetic resonance imaging and magnetic resonance spectroscopy applied in the work-up of salivary gland masses. The imaging features of different tumour types and their differential diagnoses are also discussed. Finally, staging classification and treatment options are presented.
Figures
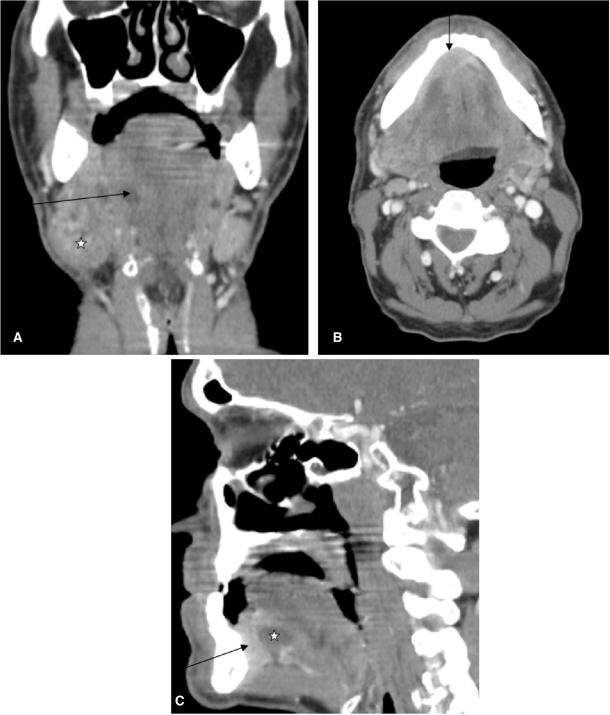
Coronal CT reconstruction (A) of a 59-year-old male patient presenting with a swelling at the angle of the mandible. Note the enlarged submandibular gland (asterisk) at the right side with dilated Wharton's duct (arrow). Axial CT scan (B) of the same patient shows a contrast enhancing mass (arrow) at the anterior floor of the mouth (squamous cell carcinoma) as aetiology of the dilated Wharton's duct and the retro-obstructive sialadenitis of the right submandibular gland. Sagittal reconstruction (C) again exemplifies the tumour at the anterior floor of the mouth (arrow) and the dilated Wharton's duct (asterisk).
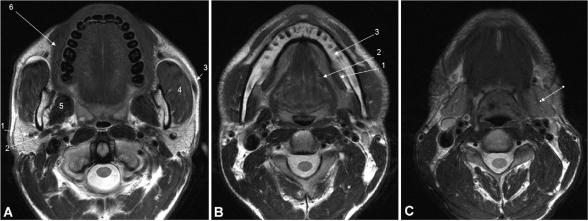
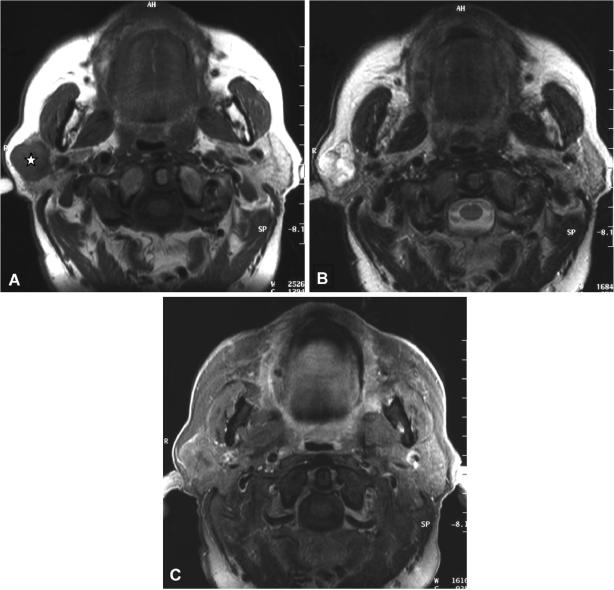
Axial T2-weighted MR image at (A) the midlevel of the parotid glands (arrows), with indications of the retromandibular vein (1), external carotid artery (2), Stensen's duct (3), masseter muscle (4), medial pterygoid muscle (5), and buccinator muscle (6). Axial T2-weighted MR image at (B) the level of the sublingual glands (arrows), with indications of mylohyoid muscle (1), hyoglossal muscle (2), and mandible (3). Axial T2-weighted MR image at (C) the level of the submandibular glands (arrows).
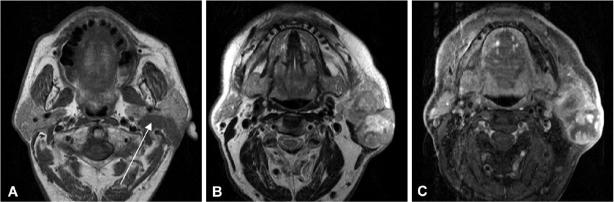
Axial T1-weighted (A), axial T2-weighted (B) and axial T1-weighted (C) contrast enhanced fat suppressed MR image of a 63-year-old male patient suffering from a carcinoma ex-pleomorphic adenoma of the left parotid gland. Please note extension into the deep parotid lobe (arrow) as well as infiltration of the subcutaneous tissue and skin. The tumour is heterogeneous on T2-weighted images (B) and shows large necrotic areas and irregular contours after contrast medium administration (C).
Axial T1-weighted MR image (A) of a 26-year-old woman with a focal lesion in her left parotid gland. Note a homogonous hypointense solid lesion with slightly irregular margins (asterisk). Axial T2-weighted MR image (B) also depicts a slightly hypointense homogeneous mass. Contrast medium enhancement with fat suppression (C) at the same level shows strong and homogenous enhancement with slightly irregular margins suspicious for malignancy. This tumour turned out to be mucoepidermoid carcinoma on histology.
Axial T2-weighted MR image (A) of a 61-year-old woman with an adenoid cystic carcinoma in the deep and superficial lobe of the right parotid gland. The tumour presents as a large heterogeneous mass. The T1-weighted contrast medium enhanced fat suppressed image (B) shows strong enhancement with hypointense areas in the centre and slightly irregular margins in the posterior part of the lesion (arrow).
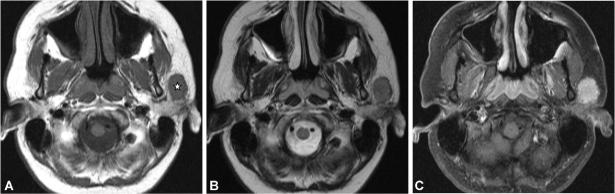
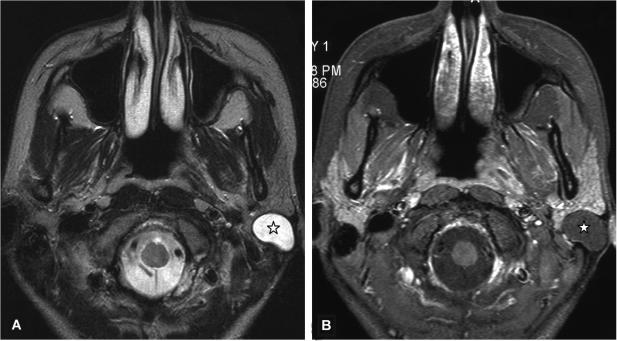
Axial T1- (A) and T2-weighted (B) MR images of a 52-year-old man with an acinic cell carcinoma of the superficial lobe of the right parotid gland (asterisk). The polylobular lesion is circumscribed and shows a hypointense signal on the T1-weighted image and a hyperintense signal on the T2-weighted image. Contrast medium enhancement (C) is only fair and the lesion shows an incomplete capsule in the posterior part.
Axial T2-weighted MR image (A) of a 73-year-old male patient with a histologically proven salivary duct carcinoma (arrows) of the deep lobe of the parotid gland displacing the superficial lobe of the parotid gland laterally. The lesion is also well delineated and hyperintense on the T1-weighted images (B) suggesting previous bleeding. Only theT1-weighted contrast-enhanced fat saturated MR image (C) reveals slightly irregular margins of the tumour, which could not be appreciated on the native images suggestive of malignancy.
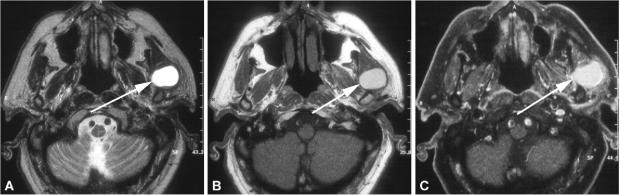
Axial T2-weighted MR image (A) of a 25-year-old woman with an epidermoid cyst in the superficial lobe (asterisk) presented as a well-delineated and homogeneous hyperintense lesion. The T1-weighted contrast-enhanced fat suppressed MR image (B) at the same level shows a homogeneous hypointense lesion without contrast medium enhancement and well-delineated margins.
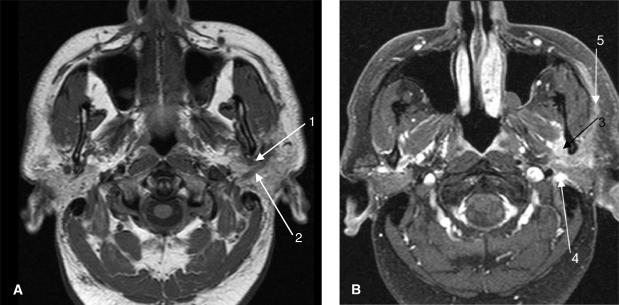
Axial non-enhanced T1-weighted MR image (A) from a 48-year-old man with facial nerve paralysis with undifferentiated carcinoma of the left parotid gland. The image demonstrates a soft tissue mass adjacent to the left mandible posteriorly that extends along the course of the auriculotemporal nerve[1] as well as the facial nerve.[2] T1-weighted contrast enhanced MR image (B) after fat suppression shows an enhancing inhomogeneous soft tissue mass with perineural spread along the auriculotemporal nerve (V3)[3] as well as the facial nerve posteriorly in the stylomastoid foramen[4] and anteriorly along the peripheral lobe of the parotid gland.[5]
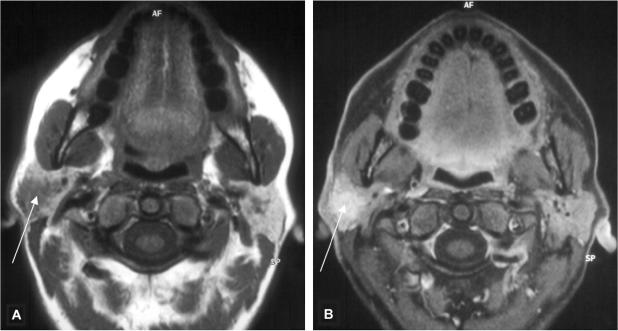
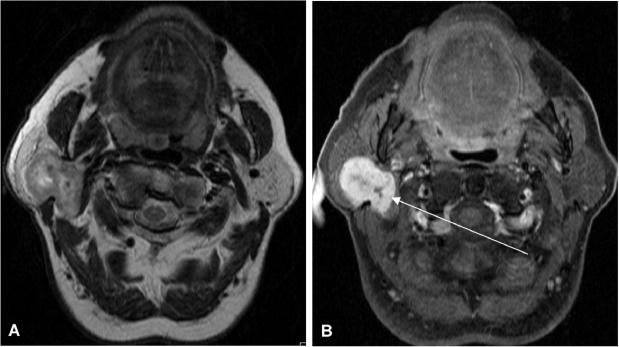
Axial T1-weighted MR image (A) of a 46-year-old women presenting with a painful lesion in the right parotid gland. A focal lesion with irregular margins can be seen (arrow). The lesion shows strong contrast medium enhancement on the fat suppressed images (B). On histology this lesion turned out to be a benign lymphoepithelial lesion (BLEL).
Similar articles
-
Digital subtraction sialography, conventional sialography, high-resolution ultrasonography and computed tomography in the diagnosis of salivary gland diseases.Eur J Radiol. 1989 Nov;9(4):224-30. Eur J Radiol. 1989. PMID: 2686991
-
Imaging of salivary gland disease.Semin Roentgenol. 2000 Jan;35(1):12-20. doi: 10.1016/s0037-198x(00)80028-0. Semin Roentgenol. 2000. PMID: 10670049 Review. No abstract available.
-
Imaging of the major salivary glands.Clin Physiol Funct Imaging. 2016 Jan;36(1):1-10. doi: 10.1111/cpf.12199. Epub 2014 Oct 16. Clin Physiol Funct Imaging. 2016. PMID: 25319072 Review.
-
Imaging of the salivary glands.Semin Roentgenol. 2013 Jan;48(1):65-74. doi: 10.1053/j.ro.2012.08.002. Semin Roentgenol. 2013. PMID: 23158051 Review. No abstract available.
-
Oral cavity, oropharynx, and salivary glands.Neuroimaging Clin N Am. 1996 May;6(2):379-400. Neuroimaging Clin N Am. 1996. PMID: 8726912 Review.
Cited by
-
Gigantic submandibular pleomorphic adenoma: A rare case report.Int J Surg Case Rep. 2019;65:91-96. doi: 10.1016/j.ijscr.2019.10.033. Epub 2019 Oct 24. Int J Surg Case Rep. 2019. PMID: 31704665 Free PMC article.
-
Clinico-histopathological review of 255 patients who underwent parotidectomy for pleomorphic adenoma: a 10-year retrospective study-a proposal for an optimal diagnostic and therapeutic algorithm for patients with recurrent pleomorphic adenoma.Eur Arch Otorhinolaryngol. 2023 Jul;280(7):3329-3335. doi: 10.1007/s00405-023-07897-y. Epub 2023 Mar 6. Eur Arch Otorhinolaryngol. 2023. PMID: 36872347 Free PMC article. Review.
-
Magnetic resonance imaging of parotid gland tumors: a pictorial essay.BMC Med Imaging. 2022 Nov 7;22(1):191. doi: 10.1186/s12880-022-00924-0. BMC Med Imaging. 2022. PMID: 36344914 Free PMC article.
-
Surgical Treatment of a Giant Pleomorphic Adenoma of the Submandibular Gland: A Case Report.Front Surg. 2022 Jan 25;8:800563. doi: 10.3389/fsurg.2021.800563. eCollection 2021. Front Surg. 2022. PMID: 35145991 Free PMC article.
-
A Case of Pleomorphic Adenoma Originating from Accessory Parotid Gland.J Maxillofac Oral Surg. 2021 Dec;20(4):573-576. doi: 10.1007/s12663-019-01241-w. Epub 2019 May 30. J Maxillofac Oral Surg. 2021. PMID: 34776686 Free PMC article. No abstract available.
References
-
- Som PM, Curtin HD. Head and neck imaging. 3rd. Vol. 2. St. Louis, MO: Mosby; 1996. pp. 877–912.
-
- Batsakis JG. Tumors of the head and neck: clinical and pathological considerations. 2nd. Baltimore, MD: Williams & Willkins; 1979. pp. 1–120.
-
- Lowe LH, Stokes LS, Johnson JE, et al. Swelling at the angle of the mandible: imaging of the pediatric parotid gland and periparotid region. Radiographics. 2001;21:1211–27. - PubMed
-
- Divi V, Fatt MA, Teknos TN, Mukherji SK. Use of cross-sectional imaging in predicting surgical location of parotid neoplasms. J Comput Assist Tomogr. 2005;29:315–19. - PubMed
-
- Freling NJ, Molenaar WM, Vermey A, et al. Malignant parotid tumors: clinical use of MR imaging and histologic correlation. Radiology. 1992;185:691–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical