

High-altitude hypoxia and preeclampsia
- PMID: 17485273
- PMCID: PMC6428070
- DOI: 10.2741/2286
High-altitude hypoxia and preeclampsia
Abstract
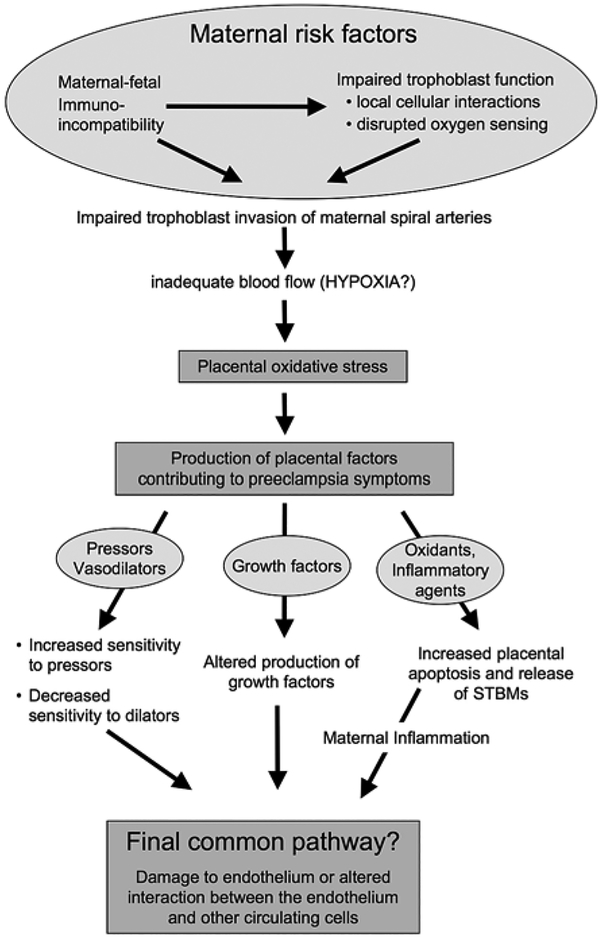
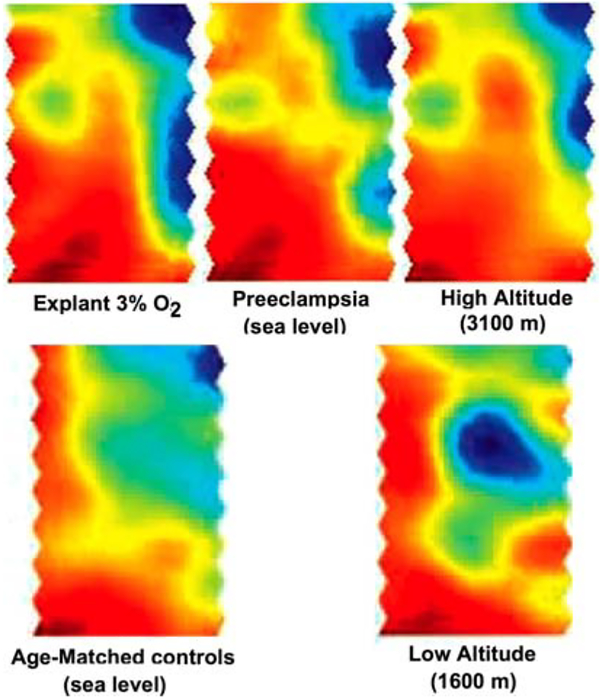
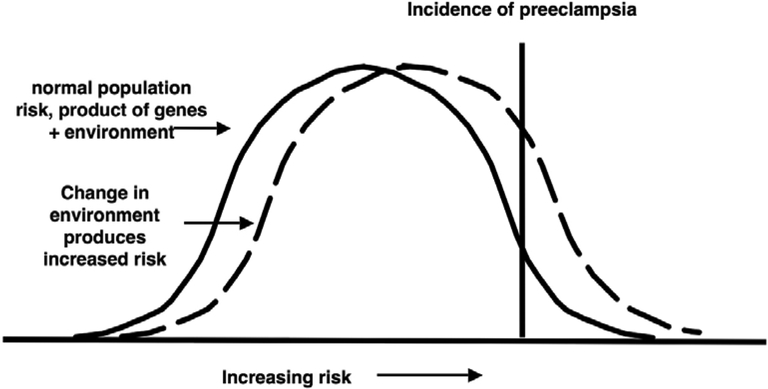
The influence of hypoxia (lowered arterial blood and/or tissue PO2) on fetoplacental development and the role of hypoxia in preeclampsia are major research foci in perinatal biology. While animal and cell models are of utility, we do not know whether artificial hypoxic stimuli mimic the pathological conditions attributed to hypoxic stress in vivo; we cannot distinguish the effects of hypoxia from under- or overlying pathologies. High altitude (>2700 m) is the natural experiment we can use to distinguish pathology from adaptation in human pregnancy. The two best known impacts of high altitude on pregnancy outcome are reduced fetal growth and an increased incidence preeclampsia. This review focuses on the mechanisms by which altitude increases maternal risk for the development of preeclampsia. The review first considers the evidence that placental hypoxia is causally involved in the development of preeclampsia. It then focuses on how data from studies of pregnant women at high altitude support (or do not support) etiological models of preeclampsia. Considered are the theories that reduced uteroplacental blood flow, circulating factors of placental origin, placental oxidative stress and increased maternal vascular reactivity are etiological in preeclampsia. The data suggest that oxidative stress and endothelial dysfunction have pathophysiological origins that are independent of placental hypoxia. We conclude that altitude shifts the individual risk for the development of preeclampsia because of impacts on multiple physiological systems, no one of which can be specifically pointed to as causal.
Figures
Similar articles
-
Pharmacological activation of peroxisome proliferator-activated receptor γ (PPAR-γ) protects against hypoxia-associated fetal growth restriction.FASEB J. 2019 Aug;33(8):8999-9007. doi: 10.1096/fj.201900214R. Epub 2019 Apr 30. FASEB J. 2019. PMID: 31039323 Free PMC article.
-
High altitude and pre-eclampsia: Adaptation or protection.Med Hypotheses. 2017 Jul;104:128-132. doi: 10.1016/j.mehy.2017.05.007. Epub 2017 May 10. Med Hypotheses. 2017. PMID: 28673571
-
High altitude during pregnancy.Clin Chest Med. 2011 Mar;32(1):21-31. doi: 10.1016/j.ccm.2010.10.008. Clin Chest Med. 2011. PMID: 21277446 Review.
-
Hypothesis: selective phosphodiesterase-5 inhibition improves outcome in preeclampsia.Med Hypotheses. 2004;63(6):1057-64. doi: 10.1016/j.mehy.2004.03.042. Med Hypotheses. 2004. PMID: 15504576
-
Vascular biology of preeclampsia.J Thromb Haemost. 2009 Mar;7(3):375-84. doi: 10.1111/j.1538-7836.2008.03259.x. J Thromb Haemost. 2009. PMID: 19087223 Review.
Cited by
-
Adverse clinical outcomes associated with sickle cell trait at high altitude.Haematologica. 2025 Feb 1;110(2):504-506. doi: 10.3324/haematol.2024.285832. Haematologica. 2025. PMID: 39363860 Free PMC article. No abstract available.
-
Elevation of Pulmonary Artery Pressure in Newborns from High-Altitude Pregnancies Complicated by Preeclampsia.Antioxidants (Basel). 2023 Feb 1;12(2):347. doi: 10.3390/antiox12020347. Antioxidants (Basel). 2023. PMID: 36829907 Free PMC article.
-
Clotting factor genes are associated with preeclampsia in high-altitude pregnant women in the Peruvian Andes.Am J Hum Genet. 2022 Jun 2;109(6):1117-1139. doi: 10.1016/j.ajhg.2022.04.014. Epub 2022 May 18. Am J Hum Genet. 2022. PMID: 35588731 Free PMC article.
-
Enhanced cellular responses and distinct gene profiles in human fetoplacental artery endothelial cells under chronic low oxygen.Biol Reprod. 2013 Dec 5;89(6):133. doi: 10.1095/biolreprod.113.110551. Print 2013 Dec. Biol Reprod. 2013. PMID: 24152727 Free PMC article.
-
Maternal Exposure to Ambient Air Pollution and Risk of Preeclampsia: A Population-Based Cohort Study in Scania, Sweden.Int J Environ Res Public Health. 2020 Mar 7;17(5):1744. doi: 10.3390/ijerph17051744. Int J Environ Res Public Health. 2020. PMID: 32155988 Free PMC article.
References
-
- Moore LG, Hershey DW, Jahnigen D & Bowes W Jr.: The incidence of pregnancy-induced hypertension is increased among Colorado residents at high altitude. Am J Obstet Gynecol 144, 423–9 (1982) - PubMed
-
- Keyes LE, Armaza JF, Niermeyer S, Vargas E, Young DA & Moore LG: Intrauterine growth restriction, preeclampsia, and intrauterine mortality at high altitude in Bolivia. Ped Res 54, 20–5 (2003) - PubMed
-
- Mahfouz AAR, El-Aid MM, Alakija W & Al-Erian RAG: Altitude and socio-biological determinants of pregnancy-associated hypertension. Int J Obstet Gynecol 44, 135–138 (1994) - PubMed
-
- Palmer SK, Moore LG, Young D, Cregger B, Berman JC & Zamudio S: Altered blood pressure course during normal pregnancy and increased preeclampsia at high altitude (3100 meters) in Colorado. Am J Obstet Gynecol 180, 1161–8 (1999) - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources