

Impact of gravity loading on post-stroke reaching and its relationship to weakness
- PMID: 17486581
- PMCID: PMC2866301
- DOI: 10.1002/mus.20817
Impact of gravity loading on post-stroke reaching and its relationship to weakness
Abstract
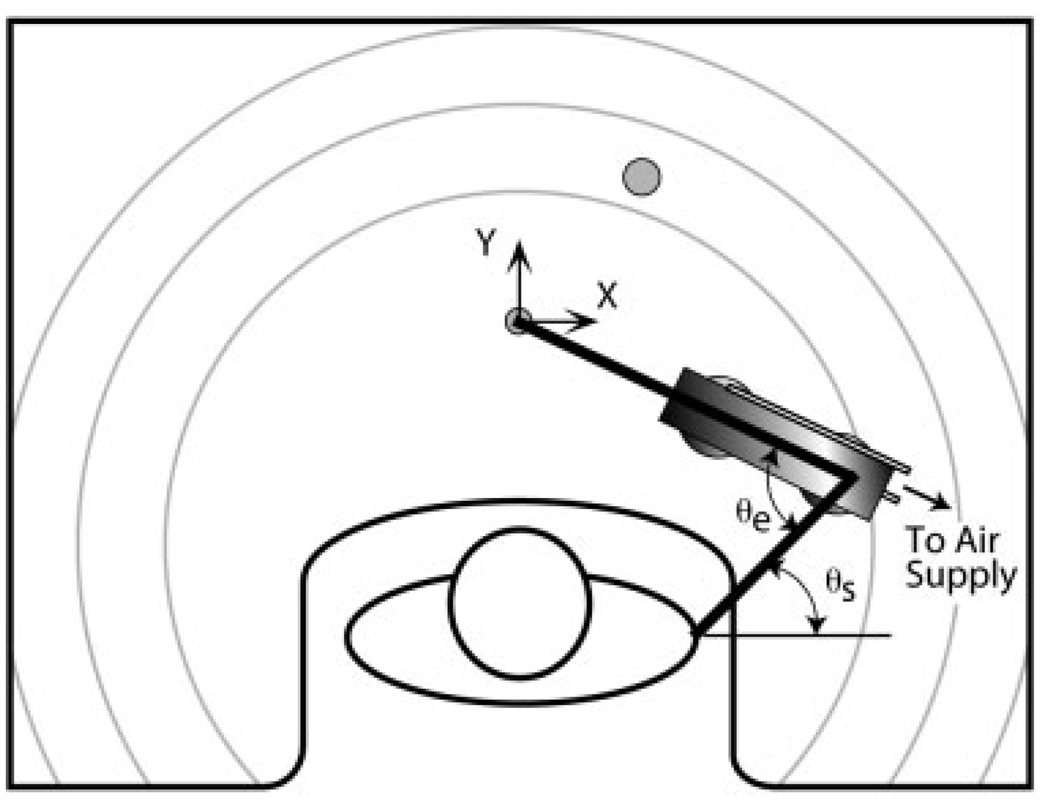
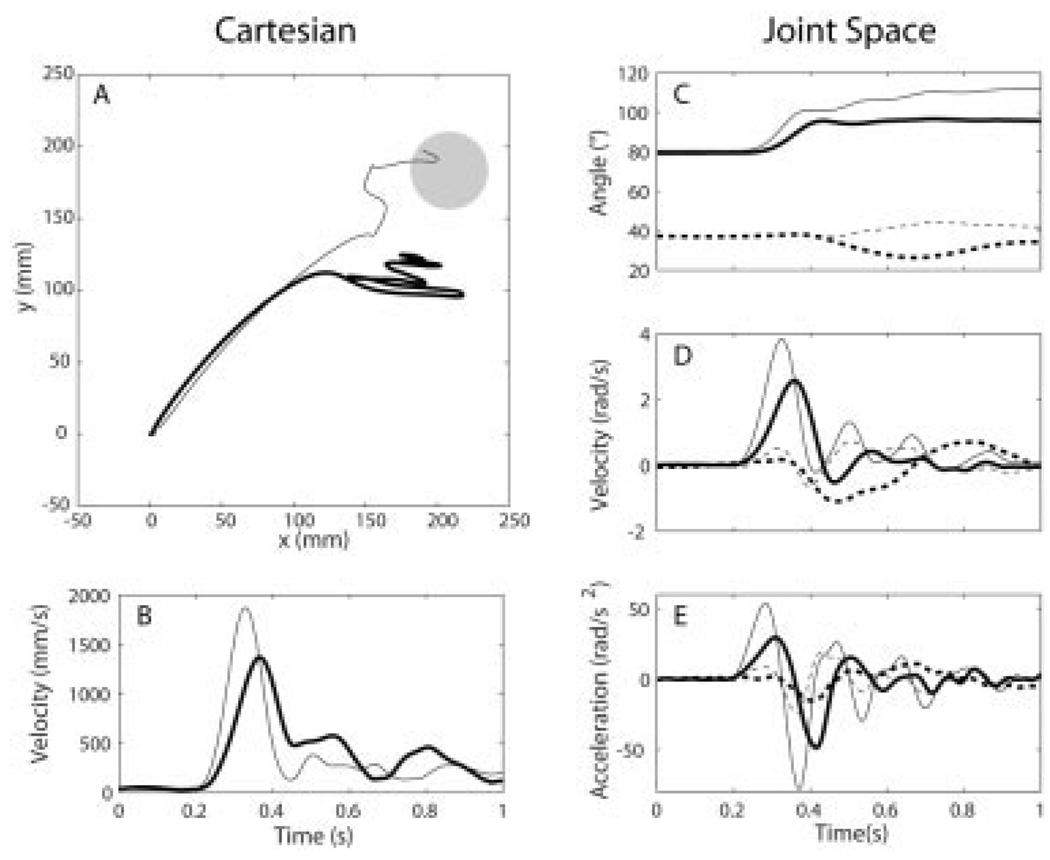
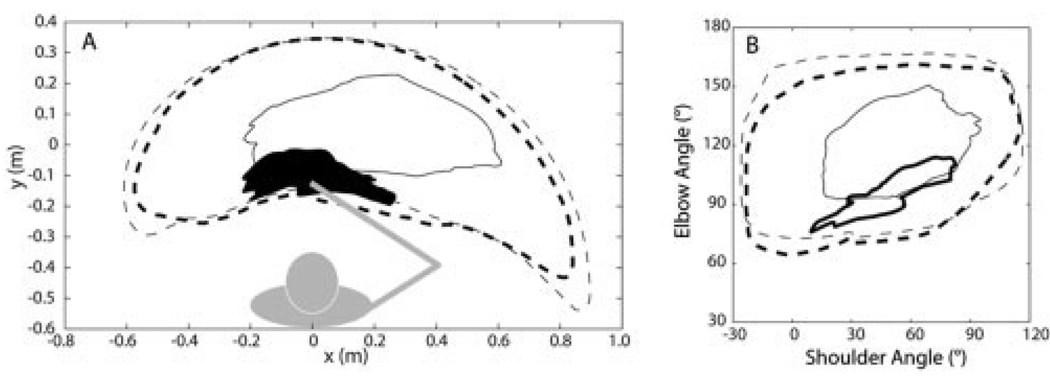
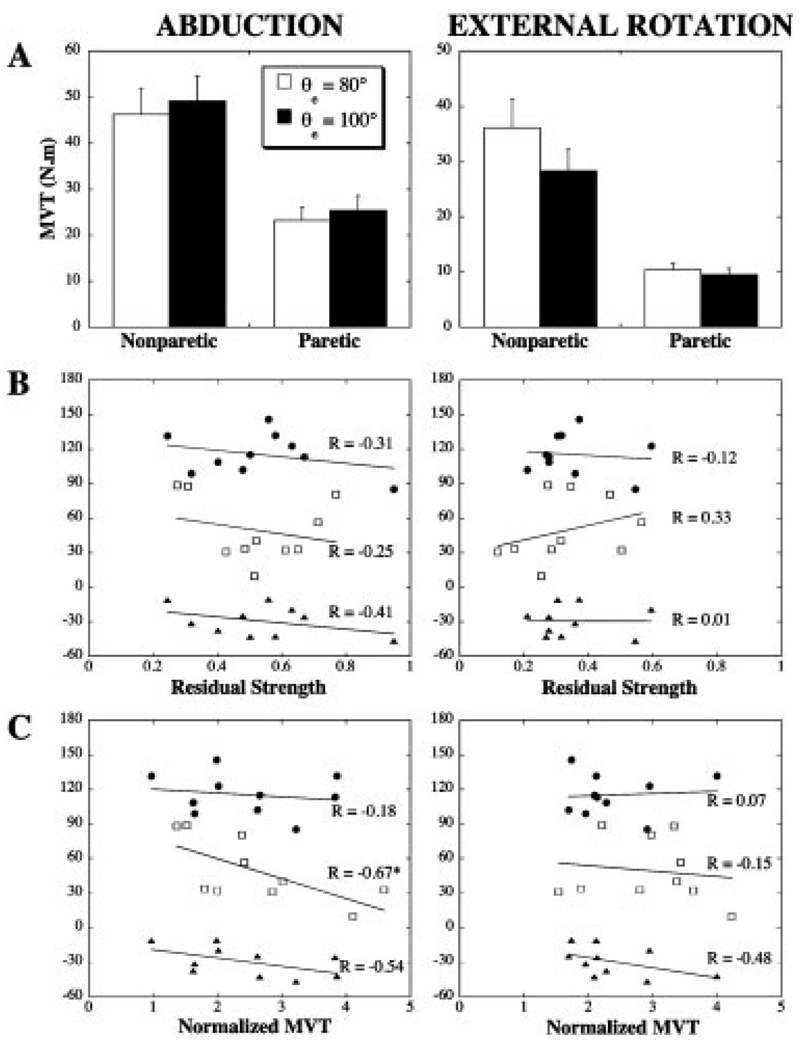
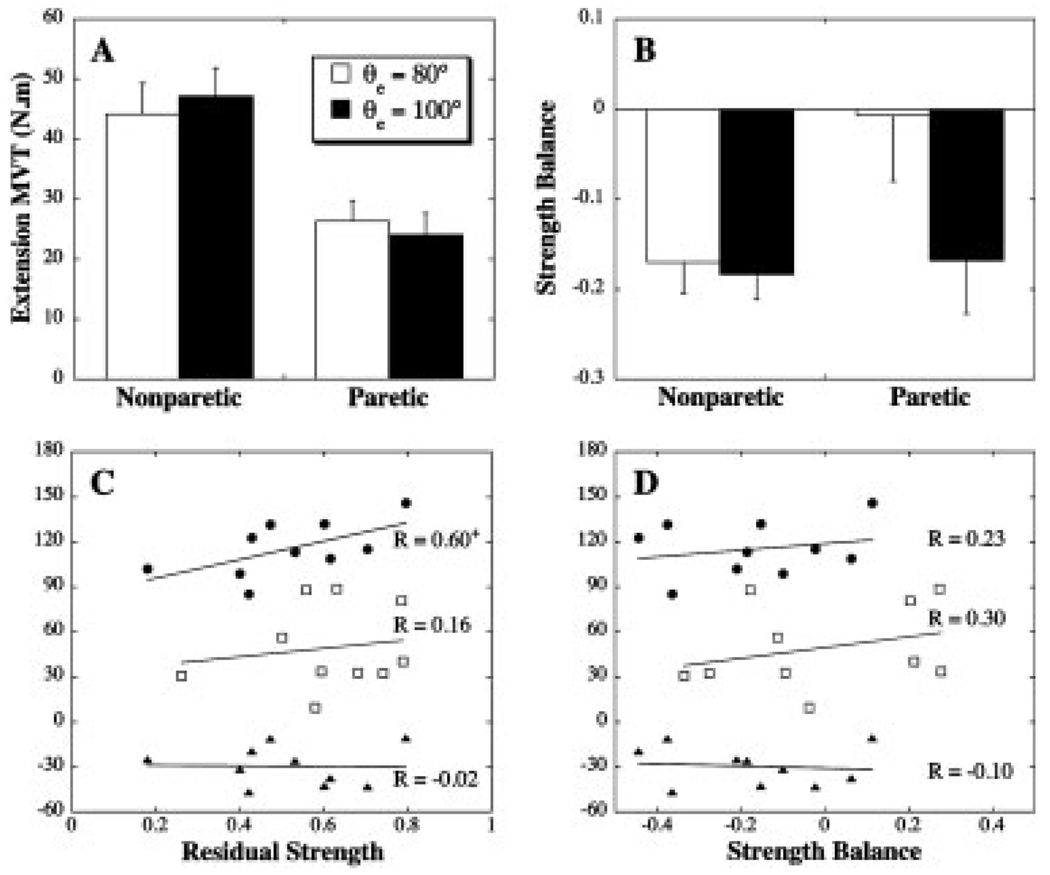
The ability to extend the elbow following stroke depends on the magnitude and direction of torques acting at the shoulder. The mechanisms underlying this link remain unclear. The purpose of this study was to evaluate whether the effects of shoulder loading on elbow function were related to weakness or its distribution in the paretic limb. Ten subjects with longstanding hemiparesis performed movements with the arm either passively supported against gravity by an air bearing, or by activation of shoulder muscles. Isometric maximum voluntary torques at the elbow and shoulder were measured using a load cell. The speed and range of elbow extension movements were negatively impacted by actively supporting the paretic limb against gravity. However, the effects of gravity loading were not related to proximal weakness or abnormalities in the elbow flexor-extensor strength balance. The findings support the existence of abnormal descending motor commands that constrain the ability of stroke survivors to generate elbow extension torque in combination with abduction torque at the shoulder.
Figures
References
-
- Barbeau H, Visintin M. Optimal outcomes obtained with body-weight support combined with treadmill training in stroke subjects. Arch Phys Med Rehabil. 2003;84:1458–1465. - PubMed
-
- Beer RF, Dewald JP, Dawson ML, Rymer WZ. Target-dependent differences between free and constrained arm movements in chronic hemiparesis. Exp Brain Res. 2004;156:458–470. - PubMed
-
- Beer RF, Dewald JP, Rymer WZ. Deficits in the coordination of multijoint arm movements in patients with hemiparesis: evidence for disturbed control of limb dynamics. Exp Brain Res. 2000;131:305–319. - PubMed
-
- Beer RF, Given JD, Dewald JP. Task-dependent weakness at the elbow in patients with hemiparesis. Arch Phys Med Rehabil. 1999;80:766–772. - PubMed
-
- Bohannon RW, Smith MB. Interrater reliability of a modified Ashworth scale of muscle spasticity. Phys Ther. 1987;67:206–207. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
