

Assessment of aortic stenosis by three-dimensional echocardiography: an accurate and novel approach
- PMID: 17488766
- PMCID: PMC1994466
- DOI: 10.1136/hrt.2006.110726
Assessment of aortic stenosis by three-dimensional echocardiography: an accurate and novel approach
Abstract
Background: Accurate assessment of aortic valve area (AVA) is important for clinical decision-making in patients with aortic valve stenosis (AS). The role of three-dimensional echocardiography (3D) in the quantitative assessment of AS has not been evaluated so far.
Objectives: To evaluate the reproducibility and accuracy of real-time three-dimensional echocardiography (RT3D) and 3D-guided two-dimensional planimetry (3D/2D) for assessment of AS, and compare these results with those of standard echocardiography and cardiac catheterisation (Cath).
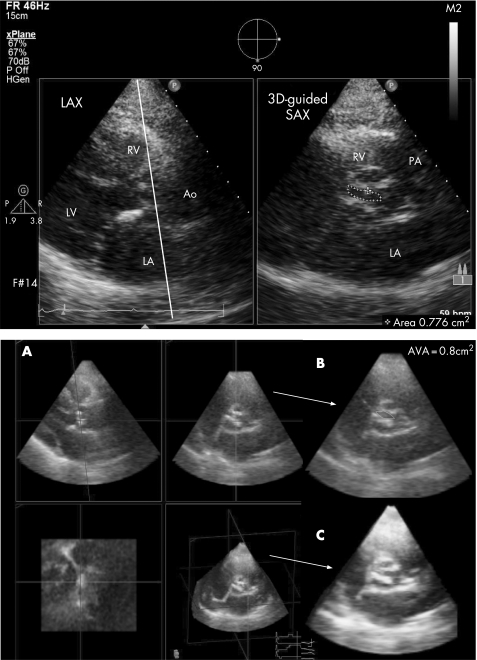
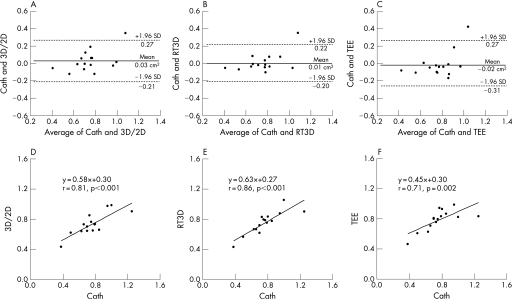
Methods: AVA was estimated by transthoracic echo-Doppler (TTE) and by direct planimetry using transoesophageal echocardiography (TEE) as well as RT3D and 3D/2D. 15 patients underwent assessment of AS by Cath.
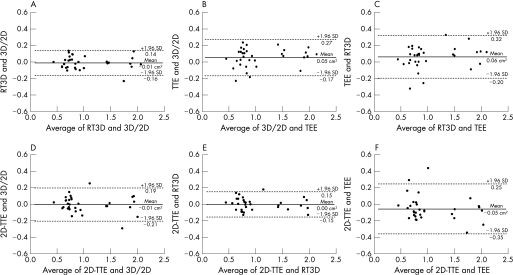
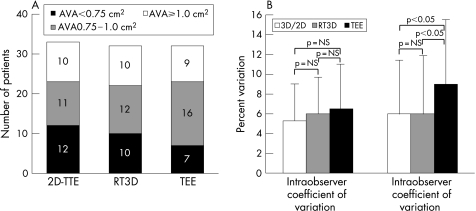
Results: 33 patients with AS were studied (20 men, mean (SD) age 70 (14) years). Bland-Altman analysis showed good agreement and small absolute differences in AVA between all planimetric methods (RT3D vs 3D/2D: -0.01 (0.15) cm(2); 3D/2D vs TEE: 0.05 (0.22) cm(2); RT3D vs TEE: 0.06 (0.26) cm(2)). The agreement between AVA assessment by 2D-TTE and planimetry was -0.01 (0.20) cm(2) for 3D/2D; 0.00 (0.15) cm(2) for RT3D; and -0.05 (0.30) cm(2) for TEE. Correlation coefficient r for AVA assessment between each of 3D/2D, RT3D, TEE planimetry and Cath was 0.81, 0.86 and 0.71, respectively. The intraobserver variability was similar for all methods, but interobserver variability was better for 3D techniques than for TEE (p<0.05).
Conclusions: The 3D echo methods for planimetry of the AVA showed good agreement with the standard TEE technique and flow-derived methods. Compared with AV planimetry by TEE, both 3D methods were at least as good as TEE and had better reproducibility. 3D aortic valve planimetry is a novel non-invasive technique, which provides an accurate and reliable quantitative assessment of AS.
Conflict of interest statement
Competing interests: None declared.
References
-
- Selzer A. Changing aspects of the natural history of valvular aortic stenosis. N Engl J Med 198731791–98. - PubMed
-
- Stewart B F, Siscovick D, Lind B K.et al Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study. J Am Coll Cardiol 199729630–634. - PubMed
-
- Bonow R O, Carabello B, Chatterjee K.et al ACC/AHA/ESC 2006 practice guidelines for the management of patients with valvular heart disease: executive summary. A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease) developed in collaboration with the Society of Cardiovascular Anesthesiologists endorsed by the Society for Cardiovascular Angiography and Interventions and the Society of Thoracic Surgeons. J Am Coll Cardiol 200648598–675. - PubMed
-
- Gorlin R, Gorlin S. Hydraulic formula for calculation of the area of the stenotic mitral valve, other cardiac valves, and central circulatory shunts. Am Heart J 1951411–18. - PubMed
-
- Skjaerpe T, Hegrenaes L, Hatle L. Non‐invasive estimation of valve area in patients with aortic stenosis by Doppler ultrasound and two‐dimensional echocardiography. Circulation 198572810–818. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials