

Exploring the association of dual use of the VHA and Medicare with mortality: separating the contributions of inpatient and outpatient services
- PMID: 17490488
- PMCID: PMC1884152
- DOI: 10.1186/1472-6963-7-70
Exploring the association of dual use of the VHA and Medicare with mortality: separating the contributions of inpatient and outpatient services
Abstract
Background: Older veterans may use both the Veterans Health Administration (VHA) and Medicare, but the association of dual use with health outcomes is unclear. We examined the association of indirect measures of dual use with mortality.
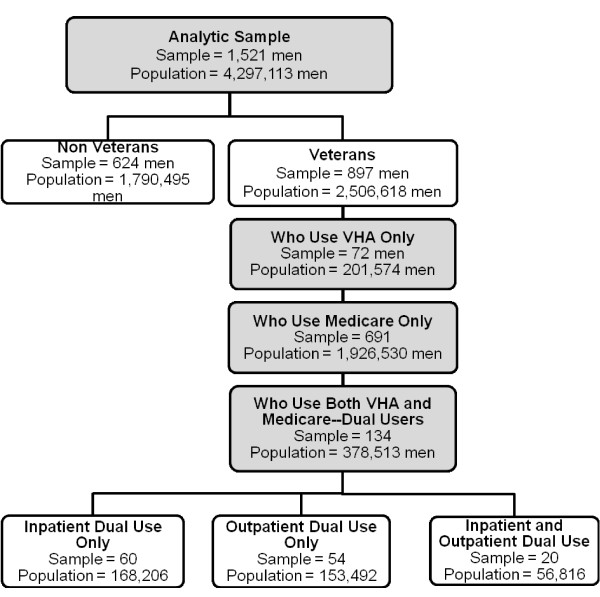
Methods: Our secondary analysis used survey, claims, and National Death Index data from the Survey on Assets and Health Dynamics among the Oldest Old. The analytic sample included 1,521 men who were Medicare beneficiaries. Veterans were classified as dual users when their self-reported number of hospital episodes or physician visits exceeded that in their Medicare claims. Veterans reporting inpatient or outpatient visits but having no Medicare claims were classified as VHA-only users. Proportional hazards regression was used.
Results: 897 (59%) of the men were veterans, of whom 134 (15%) were dual users. Among dual users, 60 (45%) met the criterion based on inpatient services, 54 (40%) based on outpatient services, and 20 (15%) based on both. 766 men (50%) died. Adjusting for covariates, the independent effect of any dual use was a 38% increased mortality risk (AHR = 1.38; p = .02). Dual use based on outpatient services marginally increased mortality risk by 45% (AHR = 1.45; p = .06), and dual use based on both inpatient and outpatient services increased the risk by 98% (AHR = 1.98; p = .02).
Conclusion: Indirect measures of dual use were associated with increased mortality risk. New strategies to better coordinate care, such as shared medical records, should be considered.
Figures
Similar articles
-
Dual use of Medicare and the Veterans Health Administration: are there adverse health outcomes?BMC Health Serv Res. 2006 Oct 9;6:131. doi: 10.1186/1472-6963-6-131. BMC Health Serv Res. 2006. PMID: 17029643 Free PMC article.
-
Risk-adjusted mortality as an indicator of outcomes: comparison of the Medicare Advantage Program with the Veterans' Health Administration.Med Care. 2006 Apr;44(4):359-65. doi: 10.1097/01.mlr.0000204119.27597.f1. Med Care. 2006. PMID: 16565637
-
Dual Medicare and Veteran Health Administration use and ambulatory care sensitive hospitalizations.J Gen Intern Med. 2011 Nov;26 Suppl 2(Suppl 2):669-75. doi: 10.1007/s11606-011-1788-4. J Gen Intern Med. 2011. PMID: 21989620 Free PMC article.
-
Veterans Health Administration and Medicare outpatient health care utilization by older rural and urban New England veterans.J Rural Health. 2005 Spring;21(2):167-71. doi: 10.1111/j.1748-0361.2005.tb00077.x. J Rural Health. 2005. PMID: 15859054
-
Gender and use of care: planning for tomorrow's Veterans Health Administration.J Womens Health (Larchmt). 2007 Oct;16(8):1188-99. doi: 10.1089/jwh.2006.0205. J Womens Health (Larchmt). 2007. PMID: 17937572 Review.
Cited by
-
Improving Transplant Medication Safety Through a Technology and Pharmacist Intervention (ISTEP): Protocol for a Cluster Randomized Controlled Trial.JMIR Res Protoc. 2019 Oct 1;8(10):e13821. doi: 10.2196/13821. JMIR Res Protoc. 2019. PMID: 31573933 Free PMC article.
-
Transitions in dual care for veterans: non-federal physician perspectives.J Community Health. 2013 Apr;38(2):225-37. doi: 10.1007/s10900-012-9604-6. J Community Health. 2013. PMID: 22903804
-
Comparison of outcomes for veterans receiving dialysis care from VA and non-VA providers.BMC Health Serv Res. 2013 Jan 18;13:26. doi: 10.1186/1472-6963-13-26. BMC Health Serv Res. 2013. PMID: 23327632 Free PMC article.
-
Dual utilization of Medicare and VA outpatient care among Veterans with spinal cord injuries and disorders.J Spinal Cord Med. 2023 Sep;46(5):716-724. doi: 10.1080/10790268.2022.2027321. Epub 2022 Feb 2. J Spinal Cord Med. 2023. PMID: 35108176 Free PMC article.
-
Veterans Health Administration enrollees' choice of care setting relates to the expansion of care options: Evidence from screening colonoscopies before and after the MISSION Act.Health Serv Res. 2024 Feb;59(1):e14241. doi: 10.1111/1475-6773.14241. Epub 2023 Sep 26. Health Serv Res. 2024. PMID: 37750415 Free PMC article.
References
-
- Selected VHA statistics: FY 2003–2004. 2005. http://www.va.gov/vhaopp/enroll01.htm Accessed July 25, 2005.
-
- Iglehart JK. The Veterans Administration medical care system faces an uncertain future. NEJM. 1985;13:1168–1171. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
