

Impact of natural killer cell dose and donor killer-cell immunoglobulin-like receptor (KIR) genotype on outcome following human leucocyte antigen-identical haematopoietic stem cell transplantation
- PMID: 17493020
- PMCID: PMC1941931
- DOI: 10.1111/j.1365-2249.2007.03360.x
Impact of natural killer cell dose and donor killer-cell immunoglobulin-like receptor (KIR) genotype on outcome following human leucocyte antigen-identical haematopoietic stem cell transplantation
Abstract
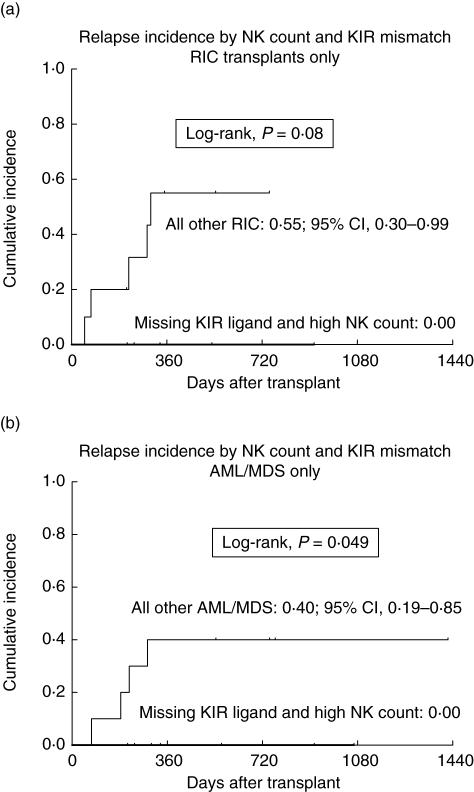
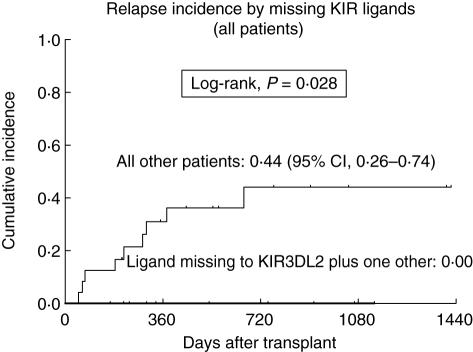
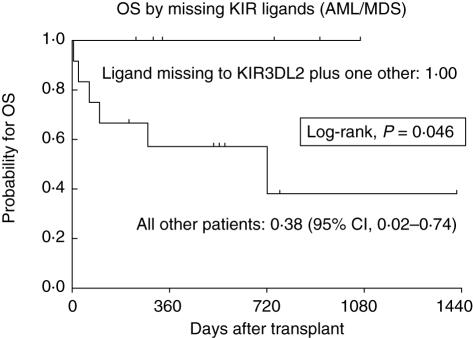
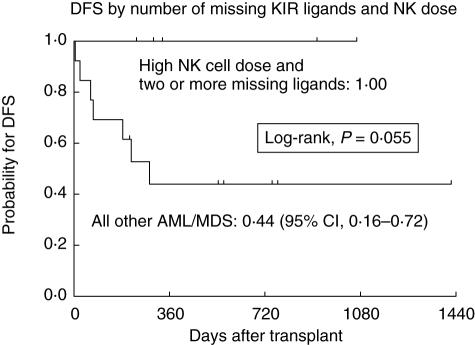
To define the role of quantitative graft composition and donor killer-cell immunoglobulin-like receptor (KIR) genotype in clinical outcome following unmanipulated peripheral blood stem cell transplantation (PBSCT) from human leucocyte antigen (HLA)-identical siblings, 43 consecutive transplants for haematological malignancies were analysed retrospectively. Twenty-four patients underwent myeloablative conditioning and 19 received busulphan/fludarabine-based reduced intensity conditioning (RIC). In patients with acute myelogenous leukaemia or myelodysplastic syndrome (AML/MDS; n = 18), no relapse occurred following transplants meeting both a high (above median) natural killer (NK) cell count and missing HLA-ligand(s) to donor's KIR(s), compared to all other AML/MDS patients (0% versus 44%; P = 0.049). Missing HLA-B and/or HLA-C ligand combined with missing HLA-A3/11 (KIR3DL2 unblocked) predicted for reduced relapse incidence regardless of diagnosis or conditioning type (P = 0.028). Moreover, in AML/MDS patients, this constellation predicted superior overall survival (OS) (P = 0.046). Transplants with more than two different activating donor KIRs were associated with an increased risk for non-relapse mortality (NRM), both by univariate and multivariate analysis. Quantitative graft composition had a significant impact exclusively in RIC transplants. Here, a trend towards reduced relapse incidence was found in patients receiving high numbers of NK cells (16% versus 54%; P = 0.09). In patients receiving high versus low T cell numbers, OS was superior (83% versus 37%; P = 0.01), due mainly to reduced NRM (0% versus 33%; P = 0.046). By multivariate analysis, relapse risk was decreased significantly in patients receiving high NK cell numbers (P = 0.039). These data suggest that both the number of transplanted NK cells and the donor KIR genotype play a role in graft-versus-malignancy mechanisms in HLA-identical PBSCT.
Figures
Similar articles
-
The role of missing killer cell immunoglobulin-like receptor ligands in T cell replete peripheral blood stem cell transplantation from HLA-identical siblings.Biol Blood Marrow Transplant. 2010 Feb;16(2):273-80. doi: 10.1016/j.bbmt.2009.10.021. Epub 2009 Oct 24. Biol Blood Marrow Transplant. 2010. PMID: 19857587
-
A defined donor activating natural killer cell receptor genotype protects against leukemic relapse after related HLA-identical hematopoietic stem cell transplantation.Leukemia. 2005 Aug;19(8):1446-51. doi: 10.1038/sj.leu.2403839. Leukemia. 2005. PMID: 15973456 Clinical Trial.
-
Donor selection for killer immunoglobulin-like receptors B haplotype of the centromeric motifs can improve the outcome after HLA-identical sibling hematopoietic stem cell transplantation.Biol Blood Marrow Transplant. 2014 Jan;20(1):98-105. Biol Blood Marrow Transplant. 2014. PMID: 24516895
-
Alloreactivity as therapeutic principle in the treatment of hematologic malignancies. Studies of clinical and immunologic aspects of allogeneic hematopoietic cell transplantation with nonmyeloablative conditioning.Dan Med Bull. 2007 May;54(2):112-39. Dan Med Bull. 2007. PMID: 17521527 Review.
-
Is there an impact of killer cell immunoglobulin-like receptors and KIR-ligand incompatibilities on outcomes after unrelated cord blood stem cell transplantation?Best Pract Res Clin Haematol. 2010 Jun;23(2):283-90. doi: 10.1016/j.beha.2010.05.005. Best Pract Res Clin Haematol. 2010. PMID: 20837340 Review.
Cited by
-
KIR and HLA genotypes are associated with disease progression and survival following autologous hematopoietic stem cell transplantation for high-risk neuroblastoma.Clin Cancer Res. 2009 Dec 1;15(23):7330-4. doi: 10.1158/1078-0432.CCR-09-1720. Epub 2009 Nov 24. Clin Cancer Res. 2009. PMID: 19934297 Free PMC article.
-
Influence of KIR and NK Cell Reconstitution in the Outcomes of Hematopoietic Stem Cell Transplantation.Front Immunol. 2020 Sep 2;11:2022. doi: 10.3389/fimmu.2020.02022. eCollection 2020. Front Immunol. 2020. PMID: 32983145 Free PMC article. Review.
-
Opportunities and limitations of natural killer cells as adoptive therapy for malignant disease.Cytotherapy. 2014 Nov;16(11):1453-1466. doi: 10.1016/j.jcyt.2014.03.009. Epub 2014 May 20. Cytotherapy. 2014. PMID: 24856895 Free PMC article. Review.
-
Breaking tolerance to self, circulating natural killer cells expressing inhibitory KIR for non-self HLA exhibit effector function after T cell-depleted allogeneic hematopoietic cell transplantation.Blood. 2009 Apr 16;113(16):3875-84. doi: 10.1182/blood-2008-09-177055. Epub 2009 Jan 28. Blood. 2009. PMID: 19179302 Free PMC article.
-
Natural killer cell education and tolerance.Cell. 2010 Sep 17;142(6):847-56. doi: 10.1016/j.cell.2010.08.031. Cell. 2010. PMID: 20850008 Free PMC article. Review.
References
-
- Rocha V, Labopin M, Gluckman E, et al. Relevance of bone marrow cell dose on allogeneic transplantation outcomes for patients with acute myeloid leukemia in first complete remission: results of a European survey. J Clin Oncol. 2002;20:4324–30. - PubMed
-
- Zaucha JM, Gooley T, Bensinger WI, et al. CD34 cell dose in granulocyte colony-stimulating factor-mobilized peripheral blood mononuclear cell grafts affects engraftment kinetics and development of extensive chronic graft-versus-host disease after human leukocyte antigen-identical sibling transplantation. Blood. 2001;98:3221–7. - PubMed
-
- Lee SH, Lee MH, Lee JH, et al. Infused CD34+ cell dose predicts long-term survival in acute myelogenous leukemia patients who received allogeneic bone marrow transplantation from matched sibling donors in first complete remission. Biol Blood Marrow Transplant. 2005;11:122–8. - PubMed
-
- Cao TM, Shizuru JA, Wong RM, et al. Engraftment and survival following reduced-intensity allogeneic peripheral blood hematopoietic cell transplantation is affected by CD8+ T-cell dose. Blood. 2005;105:2300–6. - PubMed
-
- Heimfeld S. HLA-identical stem cell transplantation: is there an optimal CD34 cell dose? Bone Marrow Transplant. 2003;31:839–45. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
