

MR angiography of dural arteriovenous fistulas: diagnosis and follow-up after treatment using a time-resolved 3D contrast-enhanced technique
- PMID: 17494662
- PMCID: PMC8134326
MR angiography of dural arteriovenous fistulas: diagnosis and follow-up after treatment using a time-resolved 3D contrast-enhanced technique
Abstract
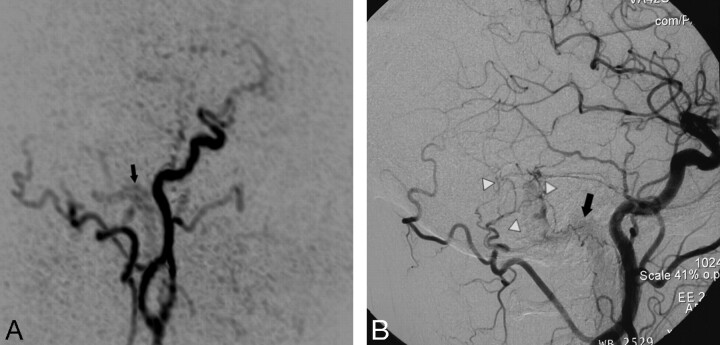
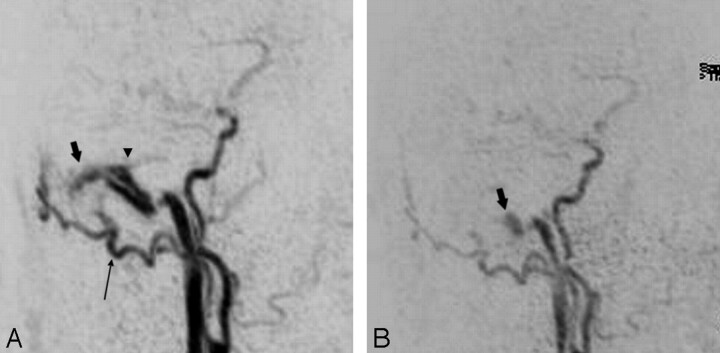
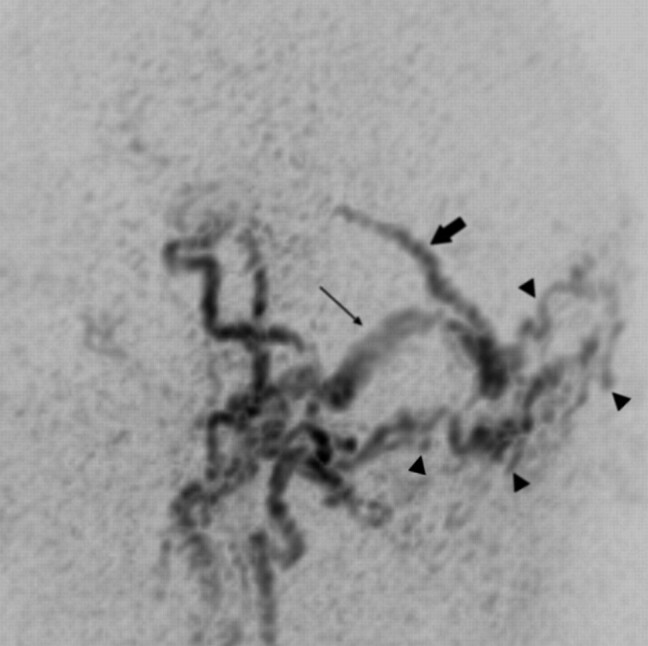
Background and purpose: Digital subtraction angiography (DSA) is the method of reference for imaging of dural arteriovenous fistula (DAVF). The goal of this study was to analyze the value of different MR images including 3D contrast-enhanced MR angiography (MRA) with a high temporal resolution in diagnostic and follow-up imaging of DAVFs.
Materials and methods: A total of 18 MR/MRA examinations from 14 patients with untreated (n=9) and/or treated (n=9) DAVFs were evaluated. Two observers assessed all MR and MRA investigations for signs indicating the presence of a DAVF, for fistula characteristics such as fistula grading, location of fistulous point, and fistula obliteration after treatment. All results were compared with DSA findings.
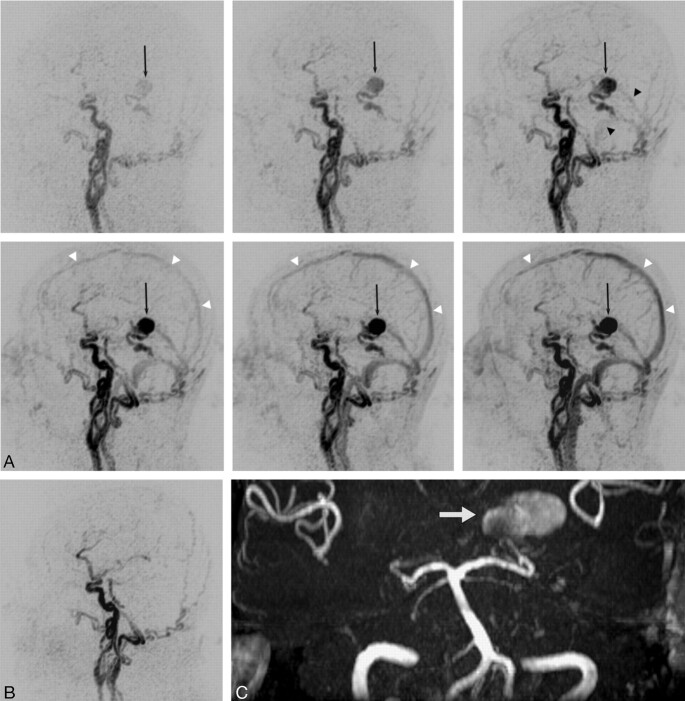
Results: On time-resolved 3D contrast-enhanced (TR 3D) MRA, the side and presence of all patent fistulas (n=13) were correctly indicated, and no false-positive findings were observed in occluded DAVFs (n=5). Grading of fistulas with this imaging technique was correct in 77% and 85% of patent fistulas for both readers, respectively. On T2-weighted images, signs indicative of a DAVF were encountered only in fistulas with cortical venous reflux (56%), whereas on 3D time-of-flight (TOF) MRA, most fistulas (88%) were correctly detected. In complete fistula occlusion, false-positive findings were encountered on both T2-weighted images and on TOF MRA images.
Conclusion: In this study, TR 3D MRA proved reliable in detecting DAVFs and suitable for follow-up imaging. The technique allowed--within limitations--to grade DAVFs. Although 3D TOF MRA can depict signs of DAVFs, its value for follow-up imaging is limited.
Figures
References
-
- Cognard C, Gobin YP, Pierot L, et al. Cerebral dural arteriovenous fistulas: clinical and angiographic correlation with a revised classification of venous drainage. Radiology 1995;194:671–80 - PubMed
-
- Davies MA, TerBrugge K, Willinsky R, et al. The validity of classification for the clinical presentation of intracranial dural arteriovenous fistulas. J Neurosurg 1996;85:830–37 - PubMed
-
- Borden JA, Wu JK, Shucart W. A proposed classification for spinal and cranial dural arteriovenous fistulous malformations and implications for treatment. J Neurosurg 1995;82:166–79 - PubMed
-
- Klisch J, Huppertz HJ, Spetzger U, et al. Transvenous treatment of carotid cavernous and dural arteriovenous fistulae: results for 31 patients and review of the literature. Neurosurgery 2003;53:836–56 - PubMed
-
- Goto K, Sidipratomo P, Ogata N, et al. Combining endovascular and neurosurgical treatments of high-risk dural arteriovenous fistulas in the lateral sinus and the confluence of sinuses. J Neurosurg 1999;90:289–99 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources