

Cisternography and ventriculography gadopentate dimeglumine-enhanced MR imaging in pediatric patients: preliminary report
- PMID: 17494664
- PMCID: PMC8134319
Cisternography and ventriculography gadopentate dimeglumine-enhanced MR imaging in pediatric patients: preliminary report
Abstract
Background and purpose: Complex CSF diseases may be underdiagnosed or poorly understood on conventional CT or MR imaging. Although intrathecal CT cisternography with water-soluble iodinated contrast medium has been used, very few studies have dealt with the intrathecal use of gadopentate dimeglumine (Gd-DTPA), though it appears superior to CT. We report our experience with the intrathecal use of Gd-DTPA for MR cisternography and ventriculography in pediatric patients referred for study and treatment of complex CSF-related diseases.
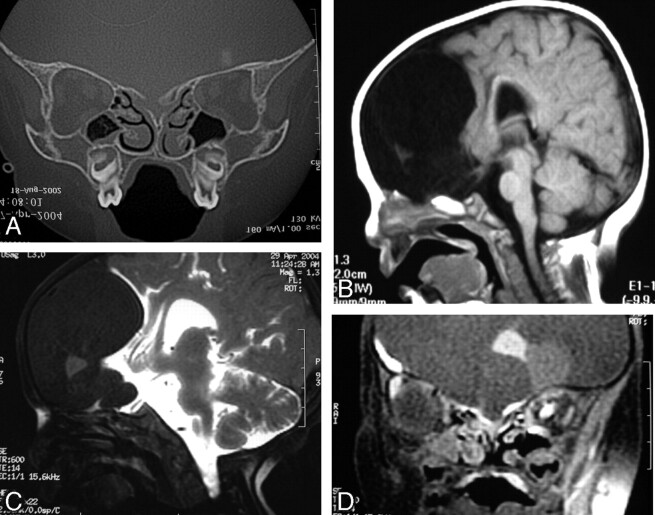
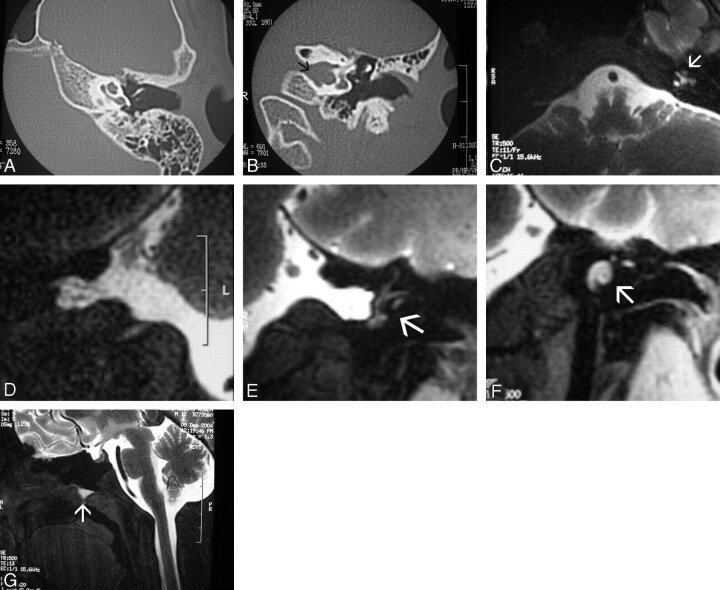
Materials and methods: Ten patients (range, 1 month-16 years of age) were selected after we obtained specific informed consent. Intrathecal gadolinium injection was performed via transfontanelle ventriculostomy, ventriculoperitoneal shunt reservoir, or lumbar puncture. Cases included spontaneous CSF leaks (n=1), complex traumatic frontoethmoidal fractures with suspected CSF leak (n=2), multiloculated congenital or acquired hydrocephalus (n=3), intraventricular tumor (n=1), suspected postoperative arachnoiditis (n=1), complex midline defect (n=1), and acquired orbital meningoencephalocele (n=1).
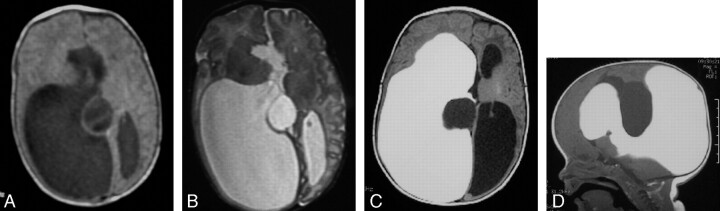
Results: No patient showed biologic, behavioral, or neurologic alterations. In complex hydrocephalus or intraventricular cysts, ventriculography Gd-DTPA MR imaging helped to differentiate isolation of a ventricle or noncommunicating cyst in all 4 patients. In suspected posttraumatic CSF leaks, the procedure established with precision the place of the leak in 1 patient and excluded it in the other. In 1 patient who underwent surgery for spinal cord neoplasm, the procedure excluded arachnoiditis. In the other 3 patients with complex CSF-related diseases, the procedure showed distinctive radiologic findings for the understanding and treatment of the disease. Altogether, in 8 patients, imaging findings influenced or changed clinical decisions and surgical planning.
Conclusions: Our preliminary results showed no side effects and potential useful clinical applications in the evaluation of CNS diseases involving the ventricular system or the subarachnoid space in selected pediatric patients.
Figures

Similar articles
-
Intrathecal gadolinium (gadopentetate dimeglumine) enhanced magnetic resonance myelography and cisternography: results of a multicenter study.Invest Radiol. 2002 Mar;37(3):152-9. doi: 10.1097/00004424-200203000-00008. Invest Radiol. 2002. PMID: 11882795
-
Intrathecal gadolinium-enhanced MR myelography and cisternography: a pilot study in human patients.AJR Am J Roentgenol. 1999 Oct;173(4):1109-15. doi: 10.2214/ajr.173.4.10511188. AJR Am J Roentgenol. 1999. PMID: 10511188
-
Intrathecal gadolinium (gadopentetate dimeglumine)-enhanced MR cisternography used to determine potential communication between the cerebrospinal fluid pathways and intracranial arachnoid cysts.Neuroradiology. 2004 Sep;46(9):744-54. doi: 10.1007/s00234-004-1240-0. Neuroradiology. 2004. PMID: 15289956 Clinical Trial.
-
Intrathecal Contrast-enhanced Computed Tomography and MR Cisternography for Skull Base Cerebrospinal Fluid Leaks and Other Intracranial Applications.Neuroimaging Clin N Am. 2025 Feb;35(1):105-121. doi: 10.1016/j.nic.2024.08.025. Epub 2024 Sep 24. Neuroimaging Clin N Am. 2025. PMID: 39521519 Review.
-
Intrathecal gadolinium-enhanced MR cisternography: a comprehensive review.AJNR Am J Neuroradiol. 2013 Jan;34(1):14-22. doi: 10.3174/ajnr.A2899. Epub 2012 Jan 19. AJNR Am J Neuroradiol. 2013. PMID: 22268089 Free PMC article. Review.
Cited by
-
The contribution of 3D-CISS and contrast-enhanced MR cisternography in detecting cerebrospinal fluid leak in patients with rhinorrhoea.Br J Radiol. 2010 Mar;83(987):225-32. doi: 10.1259/bjr/56838652. Epub 2009 Sep 1. Br J Radiol. 2010. PMID: 19723768 Free PMC article.
-
CSF otorhinorrhea in a child with inner ear dysplasia: diagnosis with T2-weighted and intrathecal contrast-enhanced MR cisternography.Jpn J Radiol. 2014 Jul;32(7):437-40. doi: 10.1007/s11604-014-0316-y. Epub 2014 Apr 23. Jpn J Radiol. 2014. PMID: 24756900
-
Surgical Repair of Skull Base CSF Leaks after Cisternography Diagnosis: Analysis of Validity and Surgical Outcome and Impact on Future Treatment Strategies.Biomed Res Int. 2022 Apr 29;2022:8740352. doi: 10.1155/2022/8740352. eCollection 2022. Biomed Res Int. 2022. PMID: 35528177 Free PMC article.
-
Children With Intracranial Arachnoid Cysts: Classification and Treatment.Medicine (Baltimore). 2015 Nov;94(44):e1749. doi: 10.1097/MD.0000000000001749. Medicine (Baltimore). 2015. PMID: 26554773 Free PMC article. Clinical Trial.
-
Intrathecal gadolinium: its time has come?AJNR Am J Neuroradiol. 2008 Jan;29(1):3-4. doi: 10.3174/ajnr.A0884. AJNR Am J Neuroradiol. 2008. PMID: 18192343 Free PMC article. No abstract available.
References
-
- Aydin K, Guven, Sencer S, et al. MRI cisternography with gadolinium-containing contrast medium: its role, advantages and limitations in the investigation of rhinorrhoea. Neuroradiology 2004;46:75–80. Epub 2003 Nov 13 - PubMed
-
- Wenzel R, Leppien A. Gadolinium-myelocisternography for cerebrospinal fluid rhinorrhoea. Neuroradiology 2000;42:874–80 - PubMed
-
- Siebner HR, Gräfin von Einsiedel H, Conrad B, et al. Magnetic resonance ventriculography with gadolinium DTPA: report of two cases. Neuroradiology 1997;39:418–22 - PubMed
-
- Zeng QY, Xiong L, Jinkins JR, et al. Intrathecal gadolinium-enhanced MR myelography and cisternography: a pilot study in human patients. AJR Am J Roentgenol 1999;173:1109–15 - PubMed
-
- Turgut TE, Ercan N, Kaymaz M, et al. Intrathecal gadolinium (gadopentetate dimeglumine)-enhanced MR cisternography used to determine potential communication between the cerebrospinal fluid pathways and intracranial arachnoid cysts. Neuroradiology 2004;46:744–54 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical