

Mechanical influences on skeletal muscle vascular tone in humans: insight into contraction-induced rapid vasodilatation
- PMID: 17495044
- PMCID: PMC2277182
- DOI: 10.1113/jphysiol.2007.131250
Mechanical influences on skeletal muscle vascular tone in humans: insight into contraction-induced rapid vasodilatation
Abstract
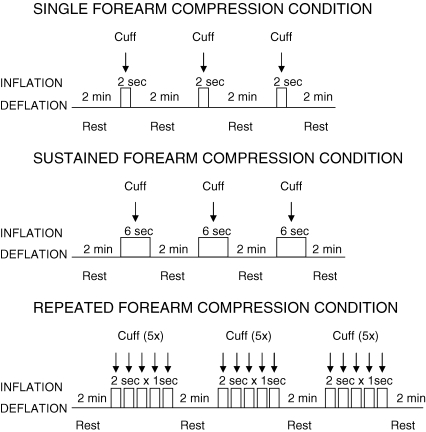
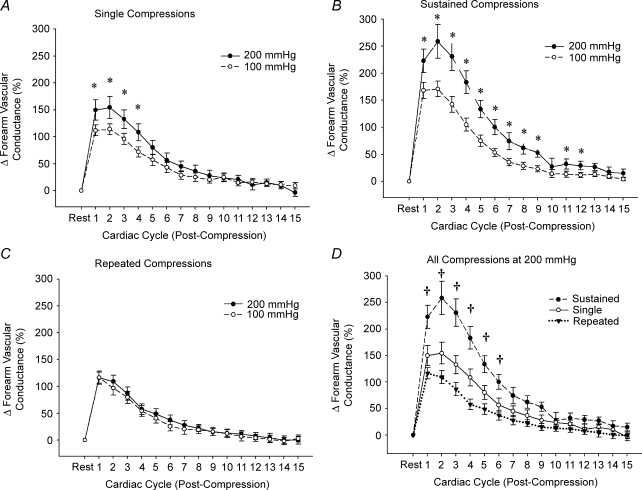
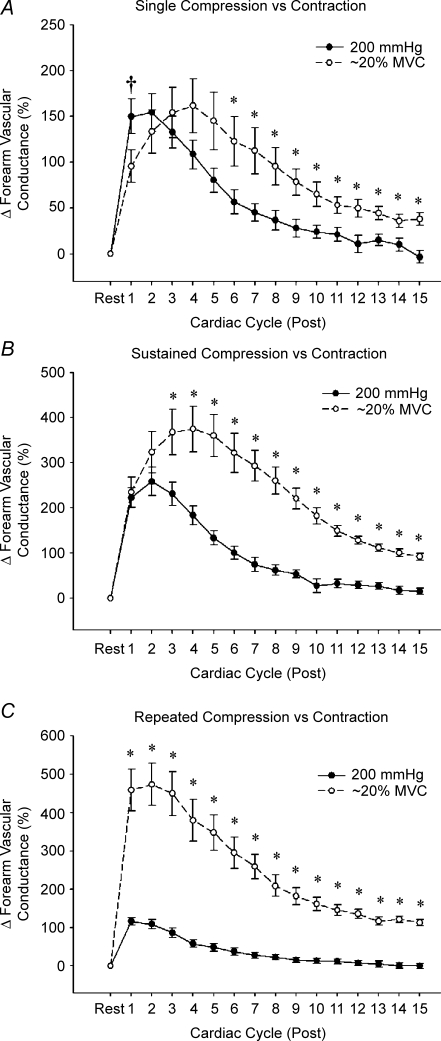
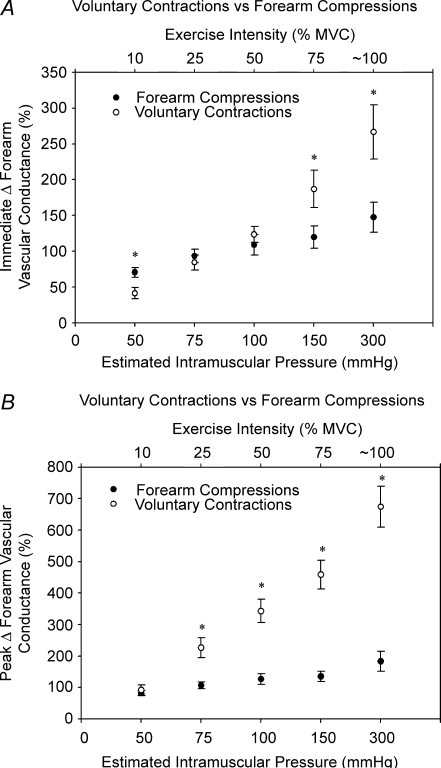
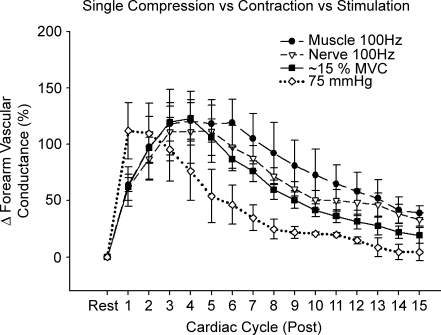
We tested the hypothesis that mechanical deformation of forearm blood vessels via acute increases in extravascular pressure elicits rapid vasodilatation in humans. In healthy adults, we measured forearm blood flow (Doppler ultrasound) and calculated forearm vascular conductance (FVC) responses to whole forearm compressions and isometric muscle contractions with the arm above heart level. We used several experimental protocols to gain insight into how mechanical factors contribute to contraction-induced rapid vasodilatation. The findings from the present study clearly indicate that acute increases in extravascular pressure (200 mmHg for 2 s) elicit a significant rapid vasodilatation in the human forearm (peak DeltaFVC approximately 155%). Brief, 6 s sustained compressions evoked the greatest vasodilatation (DeltaFVC approximately 260%), whereas the responses to single (2 s) and repeated compressions (five repeated 2 s compressions) were not significantly different (DeltaFVC approximately 155% versus approximately 115%, respectively). This mechanically induced vasodilatation peaks within 1-2 cardiac cycles, and thus is dissociated from the temporal pattern normally observed in response to brief muscle contractions ( approximately 4-7 cardiac cycles). A non-linear relation was found between graded increases in extravascular pressure and both the immediate and peak rapid vasodilatory response, such that the responses increased sharply from 25 to 100 mmHg, with no significant further dilatation until 300 mmHg (maximal DeltaFVC approximately 185%). This was in contrast to the linear intensity-dependent relation observed with muscle contractions. Our collective findings indicate that mechanical influences contribute largely to the immediate vasodilatation (first cardiac cycle) observed in response to a brief, single contraction. However, it is clear that there are additional mechanisms related to muscle activation that continue to cause and sustain vasodilatation for several more cardiac cycles after contraction. Additionally, the potential contribution of mechanical influences to the total contraction-induced hyperaemia appears greatest for low to moderate intensity single muscle contractions, and this contribution becomes less significant for sustained and repeated contractions. Nevertheless, this mechanically induced vasodilatation could serve as a feedforward mechanism to increase muscle blood flow at the onset of exercise, as well as in response to changes in contraction intensity, prior to alterations in local vasodilating substances that influence vascular tone.
Figures

Comment in
-
Feedforward vasodilatation at the onset of exercise.J Physiol. 2007 Sep 15;583(Pt 3):811. doi: 10.1113/jphysiol.2007.136846. Epub 2007 Jun 7. J Physiol. 2007. PMID: 17556386 Free PMC article. Review. No abstract available.
Similar articles
-
Evidence for impaired skeletal muscle contraction-induced rapid vasodilation in aging humans.Am J Physiol Heart Circ Physiol. 2008 Apr;294(4):H1963-70. doi: 10.1152/ajpheart.01084.2007. Epub 2008 Feb 29. Am J Physiol Heart Circ Physiol. 2008. PMID: 18310521
-
Amplification of endothelium-dependent vasodilatation in contracting human skeletal muscle: role of KIR channels.J Physiol. 2019 Mar;597(5):1321-1335. doi: 10.1113/JP276998. Epub 2018 Dec 26. J Physiol. 2019. PMID: 30506579 Free PMC article. Clinical Trial.
-
Greater post-contraction hyperaemia below vs. above heart level: the role of active vasodilatation vs. passive mechanical distension of arterioles.J Physiol. 2020 Jan;598(1):85-99. doi: 10.1113/JP278476. Epub 2019 Dec 26. J Physiol. 2020. PMID: 31654419
-
Skeletal muscle vasodilatation at the onset of exercise.J Physiol. 2007 Sep 15;583(Pt 3):825-33. doi: 10.1113/jphysiol.2007.135673. Epub 2007 Jul 5. J Physiol. 2007. PMID: 17615103 Free PMC article. Review.
-
Differential activation of sympathetic discharge to skin and skeletal muscle in humans.Acta Physiol Scand Suppl. 1997;639:1-32. Acta Physiol Scand Suppl. 1997. PMID: 9421582 Review.
Cited by
-
Passive leg movement-induced vasodilation in women: the impact of age.Am J Physiol Heart Circ Physiol. 2015 Sep;309(5):H995-H1002. doi: 10.1152/ajpheart.00422.2015. Epub 2015 Jul 17. Am J Physiol Heart Circ Physiol. 2015. PMID: 26188023 Free PMC article.
-
Intermittent pneumatic leg compressions acutely upregulate VEGF and MCP-1 expression in skeletal muscle.Am J Physiol Heart Circ Physiol. 2010 Jun;298(6):H1991-2000. doi: 10.1152/ajpheart.00006.2010. Epub 2010 Mar 26. Am J Physiol Heart Circ Physiol. 2010. PMID: 20348224 Free PMC article.
-
Understanding exercise-induced hyperemia: central and peripheral hemodynamic responses to passive limb movement in heart transplant recipients.Am J Physiol Heart Circ Physiol. 2010 Nov;299(5):H1653-9. doi: 10.1152/ajpheart.00580.2010. Epub 2010 Sep 10. Am J Physiol Heart Circ Physiol. 2010. PMID: 20833963 Free PMC article.
-
Central and peripheral contributors to skeletal muscle hyperemia: response to passive limb movement.J Appl Physiol (1985). 2010 Jan;108(1):76-84. doi: 10.1152/japplphysiol.00895.2009. Epub 2009 Nov 12. J Appl Physiol (1985). 2010. PMID: 19910331 Free PMC article.
-
Sustained exercise hyperemia during prolonged adenosine infusion in humans.Physiol Rep. 2019 Feb;7(4):e14009. doi: 10.14814/phy2.14009. Physiol Rep. 2019. PMID: 30806018 Free PMC article.
References
-
- Brock RW, Tschakovsky ME, Shoemaker JK, Halliwill JR, Joyner MJ, Hughson RL. Effects of acetylcholine and nitric oxide on forearm blood flow at rest and after a single muscle contraction. J Appl Physiol. 1998;85:2249–2254. - PubMed
-
- Buckwalter JB, Clifford PS. Autonomic control of skeletal muscle blood flow at the onset of exercise. Am J Physiol Heart Circ Physiol. 1999;277:H1872–H1877. - PubMed
-
- Burke RE. Handbook of Physiology. The Nervous System. Bethesda: American Physiological Society; 1981. Motor units: anatomy, physiology, and functional organization; pp. 345–422.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources