

The 2006 William Feinberg lecture: shifting the paradigm from stroke to global vascular risk estimation
- PMID: 17495216
- PMCID: PMC2701234
- DOI: 10.1161/STROKEAHA.106.481143
The 2006 William Feinberg lecture: shifting the paradigm from stroke to global vascular risk estimation
Abstract
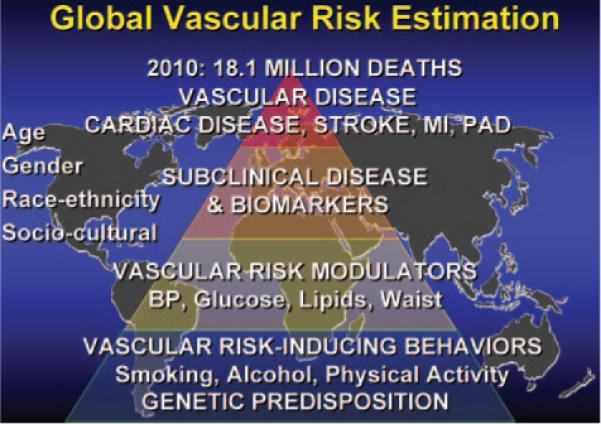
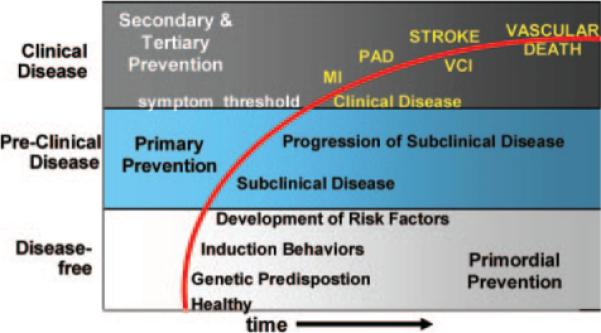
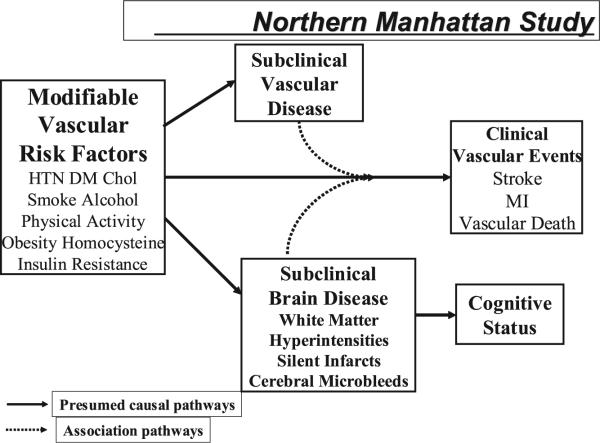
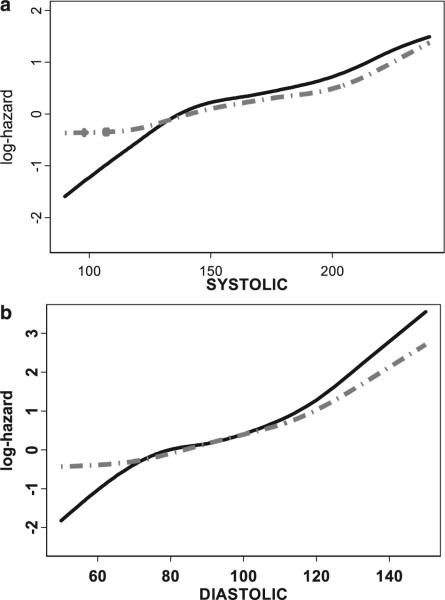
By the year 2010, it is estimated that 18.1 million people worldwide will die annually because of cardiovascular diseases and stroke. "Global vascular risk" more broadly includes the multiple overlapping disease silos of stroke, myocardial infarction, peripheral arterial disease, and vascular death. Estimation of global vascular risk requires consideration of a variety of variables including demographics, environmental behaviors, and risk factors. Data from multiple studies suggest continuous linear relationships between the physiological vascular risk modulators of blood pressure, lipids, and blood glucose rather than treating these conditions as categorical risk factors. Constellations of risk factors may be more relevant than individual categorical components. Exciting work with novel risk factors may also have predictive value in estimates of global vascular risk. Advances in imaging have led to the measurement of subclinical conditions such as carotid intima-media thickness and subclinical brain conditions such as white matter hyperintensities and silent infarcts. These subclinical measurements may be intermediate stages in the transition from asymptomatic to symptomatic vascular events, appear to be associated with the fundamental vascular risk factors, and represent opportunities to more precisely quantitate disease progression. The expansion of studies in molecular epidemiology and detection of genetic markers underlying vascular risks also promises to extend our precision of global vascular risk estimation. Global vascular risk estimation will require quantitative methods that bundle these multi-dimensional data into more precise estimates of future risk. The power of genetic information coupled with data on demographics, risk-inducing behaviors, vascular risk modulators, biomarkers, and measures of subclinical conditions should provide the most realistic approximation of an individual's future global vascular risk. The ultimate public health benefit, however, will depend on not only identification of global vascular risk but also the realization that we can modify this risk and prove the prediction models wrong.
Figures
References
-
- Sacco RL, Benjamin EJ, Broderick JP, Dyken M, Easton JD, Feinberg WM, Goldstein LB, Gorelick PB, Howard G, Kittner SJ, Manolio TA, Whisnant JP, Wolf PA. Risk Factors Panel—American Heart Association Prevention Conference IV. Stroke. 1997;28:1507–1517. - PubMed
-
- Hachinski V. The 2005 Thomas Willis Lecture. Stroke and vascular cognitive impairment: a transdisciplinary, translational and transactional approach. Stroke. 2007;38:1396. - PubMed
-
- Yusuf S, Reddy S, Ounpuu S, Anand S. Global burden of cardiovascular diseases: part I: general considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation. 2001;104:2746–2753. - PubMed
-
- Mackay J, Mensah G. The Atlas of Heart Disease and Stroke. World Health Organization in collaboration with the Centers for Disease Control and Prevention. World Health Organization; 2004. Available at: http://www.who.int/cardiovascular_diseases/resources/atlas/en/
-
- Sacco RL, Adams R, Albers G, Alberts MJ, Benavente O, Furie K, Goldstein LB, Gorelick P, Halperin J, Harbaugh R, Johnston SC, Katzan I, Kelly-Hayes M, Kenton EJ, Marks M, Schwamm LH, Tomsick T. Guidelines for prevention of stroke in patients with ischemic stroke or transient ischemic attack: a statement for healthcare professionals from the American Heart Association/American Stroke Association Council on Stroke: co-sponsored by the Council on Cardiovascular Radiology and Intervention: the American Academy of Neurology affirms the value of this guideline. Stroke. 2006;37:577–617. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
