

Helicobacter pylori in colorectal neoplasms: is there an aetiological relationship?
- PMID: 17498313
- PMCID: PMC1885433
- DOI: 10.1186/1477-7819-5-51
Helicobacter pylori in colorectal neoplasms: is there an aetiological relationship?
Abstract
Background: This pilot study was carried out to determine whether Helicobacter pylori can be detected in normal colon or in association with colorectal neoplasia.
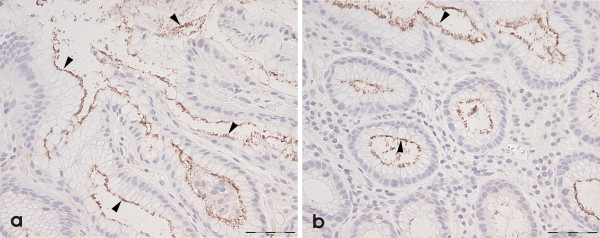
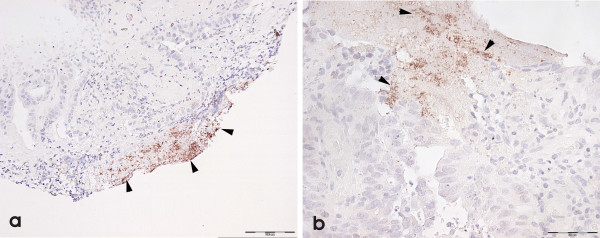
Methods: Paraffin processed colonic tissue blocks of normal colonic mucosa (n = 60), and patients diagnosed as adenoma (n = 60), and adenocarcinoma (n = 60) were retrieved from our archive; the adenoma group included tubular (n = 20), tubulovillous (n = 20) and villous adenomas (n = 20). 4 mum sections were stained by immunohistochemical methods using anti-Helicobacter pylori antibodies (polyclonal NCL-HPp and monoclonal NCL-C-jejuni).
Results: Significant numbers of Helicobacter pylori were identified in tubular adenomas (OR = 11.13; 95%CI = 1.62-76.70), tubulovillous adenomas (OR = 10.45; 95%CI = 1.52-71.52) and adenocarcinomas (OR = 8.13; 95%CI = 1.40-46.99) compared to controls: there was no association in numbers of Helicobacter pylori and villous adenomas (OR = 2.95; 95%CI = 0.29-9.96).
Conclusion: We conclude that although, in this pilot study, there appears to be an association in the prevalence of Helicobacter pylori with some, but not all, colorectal neoplasms, we can not infer causality from these results. These findings need to be further substantiated with a prospective study and the use of molecular biological techniques to determine a causal association.
Figures
Similar articles
-
Correlation between Helicobacter pylori-associated gastric diseases and colorectal neoplasia.World J Gastroenterol. 2016 May 14;22(18):4576-84. doi: 10.3748/wjg.v22.i18.4576. World J Gastroenterol. 2016. PMID: 27182167 Free PMC article.
-
Seroprevalence of Helicobacter pylori in patients with colorectal polyps and colorectal carcinoma.Am J Gastroenterol. 2001 Jan;96(1):84-8. doi: 10.1111/j.1572-0241.2001.03355.x. Am J Gastroenterol. 2001. PMID: 11197293
-
Helicobacter pylori is a risk factor for colonic neoplasms.Am J Gastroenterol. 2013 Feb;108(2):208-15. doi: 10.1038/ajg.2012.407. Epub 2012 Dec 4. Am J Gastroenterol. 2013. PMID: 23208272
-
Risk for Colorectal Neoplasia in Patients With Helicobacter pylori Infection: A Systematic Review and Meta-analysis.Clin Transl Gastroenterol. 2020 Feb;11(2):e00127. doi: 10.14309/ctg.0000000000000127. Clin Transl Gastroenterol. 2020. PMID: 32032128 Free PMC article.
-
Helicobacter pylori infection increases the risk of colorectal adenomas: cross-sectional study and meta-analysis.Dig Dis Sci. 2012 Aug;57(8):2184-94. doi: 10.1007/s10620-012-2245-x. Epub 2012 Jun 6. Dig Dis Sci. 2012. PMID: 22669208
Cited by
-
Research Progress of Intestinal Microecology in the Pathogenesis of Colorectal Adenoma and Carcinogenesis.Technol Cancer Res Treat. 2023 Jan-Dec;22:15330338221135938. doi: 10.1177/15330338221135938. Technol Cancer Res Treat. 2023. PMID: 36740990 Free PMC article. Review.
-
Laparoscopic radical resection of gastric cancer and metachronous colon cancer-a case report.Transl Cancer Res. 2020 Mar;9(3):2053-2059. doi: 10.21037/tcr.2020.01.44. Transl Cancer Res. 2020. PMID: 35117554 Free PMC article.
-
Epidemiology and risk of colorectal cancer in patients with a history of Helicobacter pylori infection: a population-based study.Ann Gastroenterol. 2023 Mar-Apr;36(2):203-207. doi: 10.20524/aog.2023.0783. Epub 2023 Feb 3. Ann Gastroenterol. 2023. PMID: 36864940 Free PMC article.
-
Clinicopathologic features of gastric cancer with synchronous and metachronous colorectal cancer in Korea: are microsatellite instability and p53 overexpression useful markers for predicting colorectal cancer in gastric cancer patients?Gastric Cancer. 2016 Jul;19(3):798-807. doi: 10.1007/s10120-015-0552-6. Epub 2015 Oct 7. Gastric Cancer. 2016. PMID: 26445944
-
Gut Microbiota in Colorectal Cancer: Biological Role and Therapeutic Opportunities.Cancers (Basel). 2023 Jan 30;15(3):866. doi: 10.3390/cancers15030866. Cancers (Basel). 2023. PMID: 36765824 Free PMC article. Review.
References
-
- Cummings OW. Pathology of the adenoma-carcinoma sequence: from aberrant crypt focus to invasive carcinoma. Semin Gastrointest Dis. 2000;11:229–237. - PubMed
-
- Day DW, Jass JR, Price AB, Shepherd NA, Sloan JM, Talbot IC, Warren BF, Williams GT. Morson and Dawson's gastrointestinal pathology. 4th. Oxford, Blackwell Science Ltd; 2003.
-
- Liu C, Crawford JM. The gastrointestinal tract. In: Kumar V, Abbas AK and Fausto N, editor. Robbins and Cotran Pathologic Basis of Disease. 7th. Philadelphia, Elsevier Saunders; 2005. pp. 797–875.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
