

Combination of psychotherapy and benzodiazepines versus either therapy alone for panic disorder: a systematic review
- PMID: 17501985
- PMCID: PMC1894782
- DOI: 10.1186/1471-244X-7-18
Combination of psychotherapy and benzodiazepines versus either therapy alone for panic disorder: a systematic review
Abstract
Background: The efficacy of combined psychotherapy and benzodiazepine treatment for panic disorder is still unclear despite its widespread use. The present systematic review aims to examine its efficacy compared with either monotherapy alone.
Methods: All randomised trials comparing combined psychotherapy and benzodiazepine for panic disorder with either therapy alone were identified by comprehensive electronic search on the Cochrane Registers, by checking references of relevant studies and of other reviews, and by contacting experts in the field. Two reviewers independently checked eligibility of trials, assessed quality of trials and extracted data from eligible trials using a standardized data extraction form. Our primary outcome was "response" defined by global judgement. Authors of the original trials were contacted for further unpublished data. Meta-analyses were undertaken synthesizing data from all relevant trials.
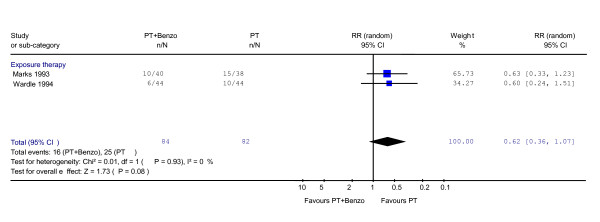
Results: Only two studies, which compared the combination with behaviour (exposure) therapy, met our eligibility criteria. Both studies had a 16-week intervention. Unpublished data were retrieved for one study. The relative risk for response for the combination was 1.25 (95%CI: 0.78 to 2.03) during acute phase treatment, 0.78 (0.45 to 1.35) at the end of treatment, and 0.62 (0.36 to 1.07) at 6-12 months follow-up. Some secondary outcomes hinted at superiority of the combination during acute phase treatment. One study was identified comparing the combination to benzodiazepine. The relative risk for response was 1.57 (0.83 to 2.98), 3.39 (1.03 to 11.21, statistically significant) and 2.31 (0.79 to 6.74) respectively. The superiority of the combination was observed on secondary outcomes at all the time points. No sub-group analyses were conducted due to the limited number of included trials.
Conclusion: Unlike some narrative reviews in the literature, our systematic search established the paucity of high quality evidence for or against the combined psychotherapy plus benzodiazepine therapy for panic disorder. Based on limited available published and unpublished data, however, the combined therapy is probably to be recommended over benzodiazepine alone for panic disorder with agoraphobia. The combination might be superior to behaviour therapy alone during the acute phase, but afterwards this trend may be reversed. We know little from these trials about their adverse effects.
Figures





References
-
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen HU, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Results from the National Comorbidity Survey. Arch Gen Psychiatry. 1994;51:8–19. - PubMed
-
- Beck AT, Sokol L, Clark DA, Berchick R, Wright F. A crossover study of focused cognitive therapy for panic disorder. Am J Psychiatry. 1992;149:778–783. - PubMed
-
- American Psychiatric Association Practice guideline for the treatment of patients with panic disorder. Work Group on Panic Disorder. Am J Psychiatry. 1998;155:1–34. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
