

Acute and long-term survival in chronically critically ill surgical patients: a retrospective observational study
- PMID: 17504535
- PMCID: PMC2206407
- DOI: 10.1186/cc5915
Acute and long-term survival in chronically critically ill surgical patients: a retrospective observational study
Abstract
Introduction: Various cohort studies have shown that acute (short-term) mortality rates in unselected critically ill patients may have improved during the past 15 years. Whether these benefits also affect acute and long-term prognosis in chronically critically ill patients is unclear, as are determinants relevant to prognosis.
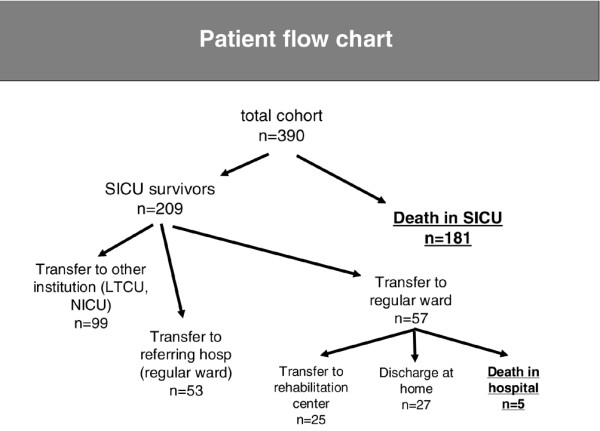
Methods: We conducted a retrospective analysis of data collected from March 1993 to February 2005. A cohort of 390 consecutive surgical patients requiring intensive care therapy for more than 28 days was analyzed.
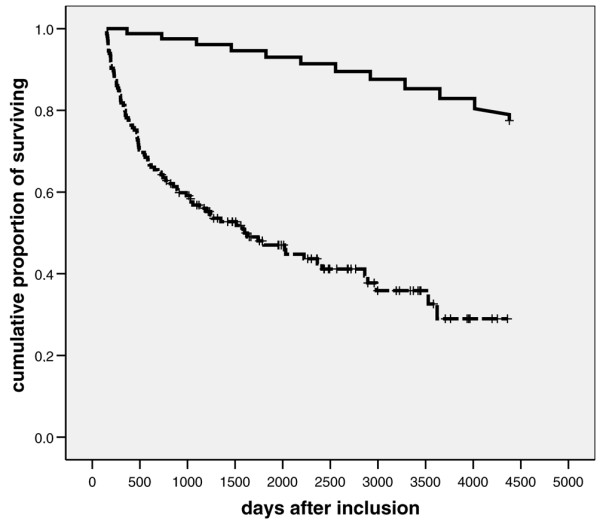
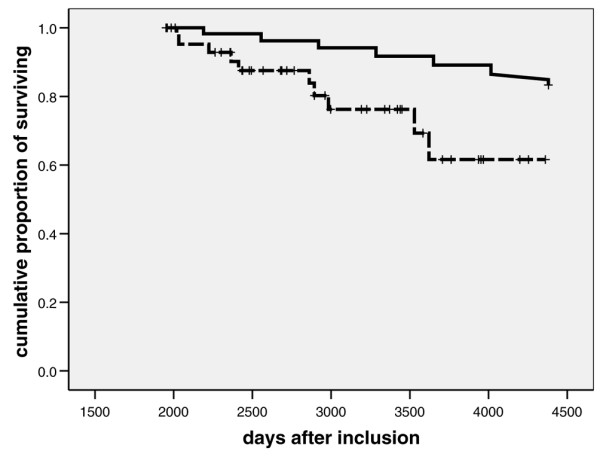
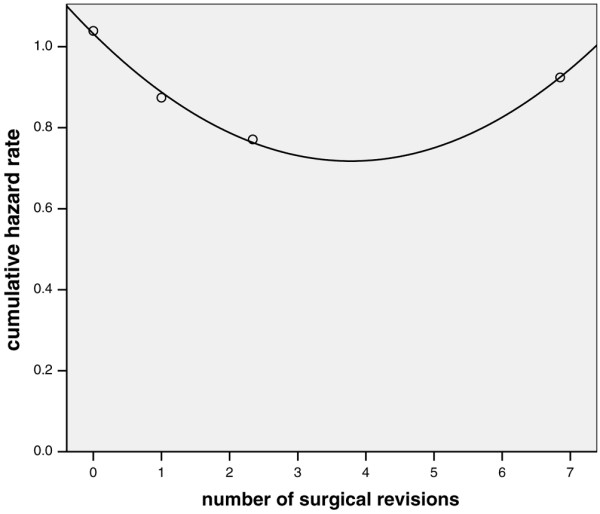
Results: The intensive care unit (ICU) survival rate was 53.6%. Survival rates at one, three and five years were 61.8%, 44.7% and 37.0% among ICU survivors. After adjustment for relevant covariates, acute and long-term survival rates did not differ significantly between 1993 to 1999 and 1999 to 2005 intervals. Acute prognosis was determined by disease severity during ICU stay and by primary diagnosis. However, only the latter was independently associated with long-term prognosis. Advanced age was an independent prognostic determinant of poor short-term and long-term survival.
Conclusion: Acute and long-term prognosis in chronically critically ill surgical patients has remained unchanged throughout the past 12 years. After successful surgical intervention and intensive care, long-term outcome is reasonably good and is mainly determined by age and underlying disease.
Figures
References
-
- Hartl WH, Wolf H, Schneider CP, Küchenhoff H, Jauch KW. Secular trends in mortality associated with new therapeutic strategies in surgical critical illness. Am J Surg. 2007. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
