

Hepatic portal venous gas: a report of two cases and a review of the epidemiology, pathogenesis, diagnosis and approach to management
- PMID: 17505567
- PMCID: PMC2657713
- DOI: 10.1155/2007/934908
Hepatic portal venous gas: a report of two cases and a review of the epidemiology, pathogenesis, diagnosis and approach to management
Abstract
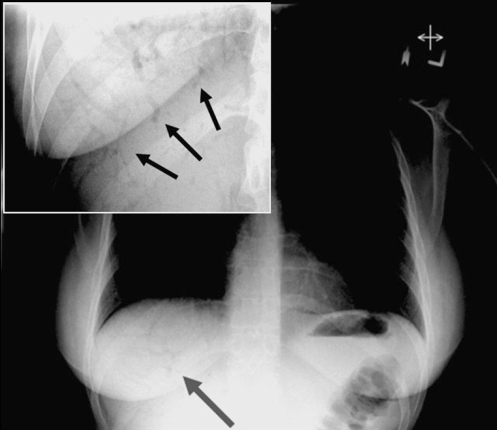
Background: Hepatic portal venous gas (HPVG) is a rare condition that occurs when intraluminal gas and/or gas produced by intestinal bacteria enters the portal venous circulation. The most common precipitating factors include ischemia, intra-abdominal abscesses and inflammatory bowel disease. However, HPVG has recently been recognized as a rare complication of endoscopic and radiological procedures. Earlier studies advised immediate surgical intervention, but according to current recommendations, in some settings, HPVG can be managed conservatively. The present study reports two cases of HPVG; one that occurred following colonoscopy in a patient with severe Crohn's disease and one in a patient with graft-versus-host disease.
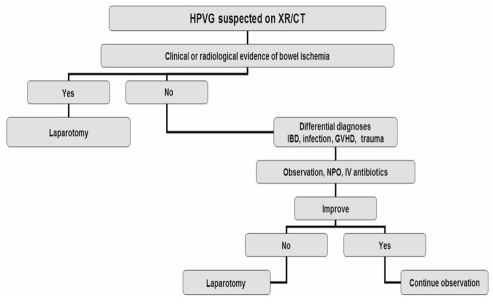
Methods: The epidemiology, pathogenesis, diagnosis and management of HPVG are reviewed. Two case reports are presented, followed by the development of a management algorithm.
Results: Of the two patients that developed HPVG, one was an outpatient undergoing a colonoscopy for assessment of Crohn's disease activity and the other was an inpatient with graft-versus-host disease. Once the diagnosis of HPVG was made, both patients were managed conservatively with antibiotic therapy and management of their underlying disease.
Conclusions: HPVG can occur in the setting of severe gastrointestinal disease states and following endoscopic procedures. It is critical that gastroenterologists are aware of the differential diagnosis, pathogenesis, diagnostic approach and management of HPVG.
HISTORIQUE :: La présence de gaz dans la veine porte hépatique (GVPH) est rare et survient lorsque des gaz intraluminaux et/ou produits par des bactéries intestinales pénètrent la circulation de la veine porte. Les facteurs déclencheurs les plus courants sont l’ischémie, les abcès intra-abdominaux et la maladie inflammatoire de l’intestin. Par contre, la présence de GVPH a récemment été reconnue comme une complication rare des interventions endoscopiques et radiologiques. Des études antérieures préconisaient une intervention chirurgicale immédiate, mais selon les recommandations actuelles, dans certains contextes, la présence de GVPH peut être traitée de manière conservatrice. La présente étude signale deux cas de GVPH, l’un survenu après une colonoscopie chez un patient atteint de maladie de Crohn avancée, et l’autre, chez un patient ayant présenté un rejet de greffe.
MÉTHODE :: L’épidémiologie, la pathogenèse, le diagnostic et le traitement du GVPH sont passés en revue ici. Deux rapports de cas sont présentés suivis d’un algorithme thérapeutique.
RÉSULTATS :: Des deux patients ayant développé un problème de GVPH, l’un était un patient non hospitalisé qui subissait une coloscopie pour évaluation de l’activité de sa maladie de Crohn et l’autre était un patient hospitalisé qui présentait un rejet de greffe. Une fois le diagnostic de GVPH posé, les deux patients ont été traités de manière conservatrice par antibiothérapie et traitement de la maladie sous-jacente.
CONCLUSION :: La présence de GVPH peut se manifester dans le contexte de graves maladies digestives et après des interventions endoscopiques. Il est important de sensibiliser les gastro-entérologues au diagnostic différentiel, à la pathogenèse, à l’approche diagnostique et au traitement des problèmes de GVPH.
Figures

References
-
- Buras R, Guzzetta P, Avery G, Naulty C. Acidosis and hepatic portal venous gas: Indications for surgery in necrotizing enterocolitis. Pediatrics. 1986;78:273–7. - PubMed
-
- King S, Shuckett B. Sonographic diagnosis of portal venous gas in two pediatric liver transplant patients with benign pneumatosis intestinalis. Case reports and literature review. Pediatr Radiol. 1992;22:577–8. - PubMed
-
- Kurbegov AC, Sondheimer JM. Pneumatosis intestinalis in non-neonatal pediatric patients. Pediatrics. 2001;108:402–6. - PubMed
-
- Rehan VK, Seshia MM, Johnston B, Reed M, Wilmot D, Cook V. Observer variability in interpretation of abdominal radiographs of infants with suspected necrotizing enterocolitis. Clin Pediatr (Phila) 1999;38:637–43. - PubMed
-
- See C, Elliott D. Images in clinical medicine. Pneumatosis intestinalis and portal venous gas. N Engl J Med. 2004;350:e3. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources