

A pharmacokinetic model for L-carnitine in patients receiving haemodialysis
- PMID: 17506778
- PMCID: PMC2000652
- DOI: 10.1111/j.1365-2125.2007.02926.x
A pharmacokinetic model for L-carnitine in patients receiving haemodialysis
Abstract
Aims: Patients requiring chronic haemodialysis may develop a secondary carnitine deficiency through dialytic loss of L-carnitine. A previous report has described the plasma concentrations of L-carnitine in 12 such patients under baseline conditions and after L-carnitine administration (20 mg kg(-1)). A three-compartment pharmacokinetic model was developed to describe these data to make inferences about carnitine supplementation in these patients.
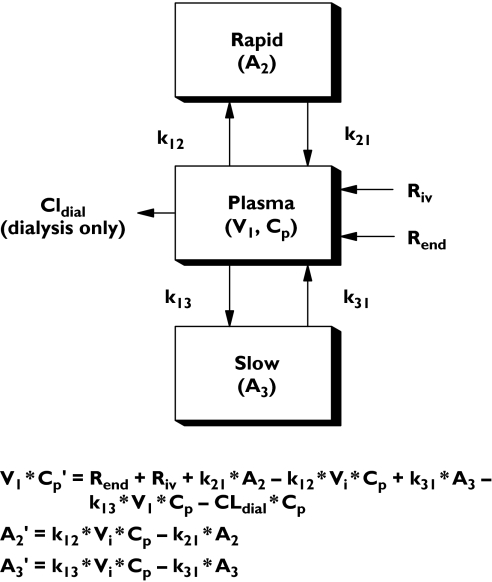
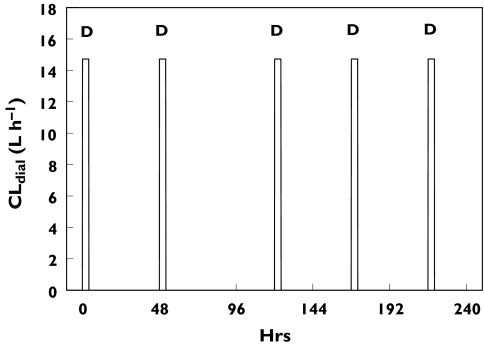
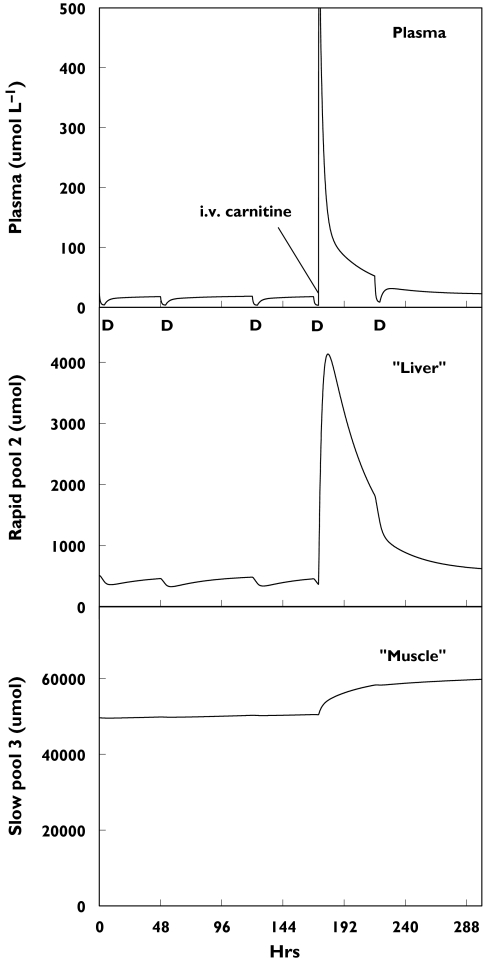
Methods: L-carnitine removal was mediated solely by intermittent haemodialysis, which was incorporated into the model as an experimentally derived dialysis clearance value that was linked to an on-off pulse function. Data were described by a model with a central compartment linked to 'fast'- and 'slow'-equilibrating peripheral compartments.
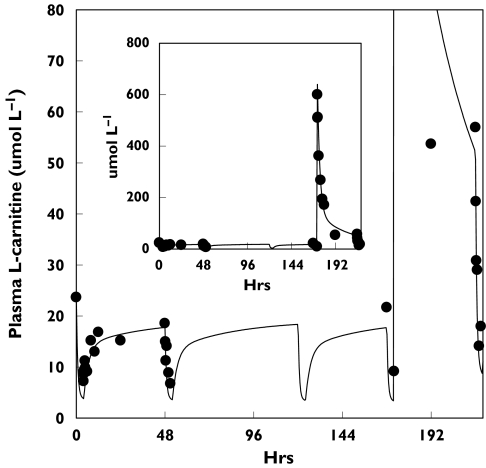
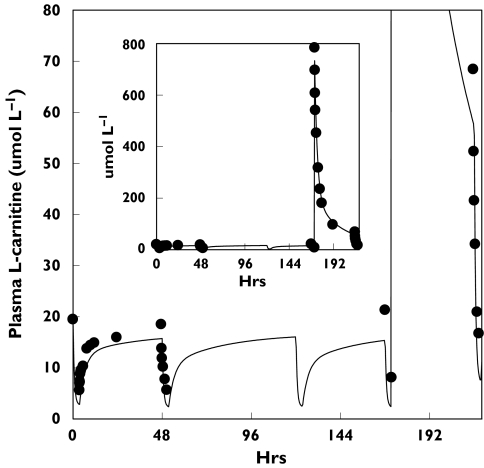
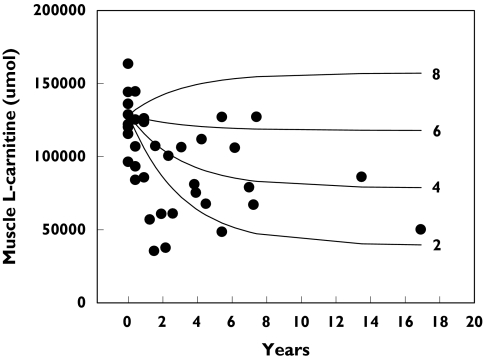
Results: The model adequately described the changing plasma concentrations of endogenous L-carnitine in individual haemodialysis patients. Based on pooled data (mean +/- SD; n = 12), the volume of the central compartment was 10.09 +/- 0.72 l and the transfer rate constants into and out of the slowly equilibrating pool were 0.100 +/- 0.018 h(-1) and 0.00014 +/- 0.00016 h(-1), respectively. The turnover time of L-carnitine in the slow pool (which was assumed to represent muscle) was approximately 300 days. The model was in general agreement with separate data on the measured loss of carnitine from muscle in dialysis patients.
Conclusions: Haemodialysis causes rapid reductions in plasma L-carnitine concentrations with each dialysis session. Plasma concentrations are restored between sessions by redistribution from peripheral compartments. However, during chronic haemodialysis, the ongoing dialytic loss of L-carnitine may lead to a slow depletion of the compound, contributing to a possible secondary deficiency.
Figures
References
-
- Bremer J. Carnitine – metabolism and functions. Physiol Rev. 1983;63:1420–80. - PubMed
-
- Rebouche CJ. Kinetics, pharmacokinetics, and regulation of L-carnitine and acetyl-L-carnitine metabolism. Ann NY Acad Sci. 2004;1033:30–41. - PubMed
-
- Evans AM, Fornasini G. Pharmacokinetics of L-carnitine. Clin Pharmacokinet. 2003;42:941–67. - PubMed
-
- Ahmad S. L-carnitine in dialysis patients. Semin Dialysis. 2001;14:209–17. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
