

Population pharmacokinetics-pharmacodynamics of alemtuzumab (Campath) in patients with chronic lymphocytic leukaemia and its link to treatment response
- PMID: 17506867
- PMCID: PMC2000651
- DOI: 10.1111/j.1365-2125.2007.02914.x
Population pharmacokinetics-pharmacodynamics of alemtuzumab (Campath) in patients with chronic lymphocytic leukaemia and its link to treatment response
Abstract
Aims: To characterize alemtuzumab pharmacokinetics and its exposure-response relationship with white blood cell (WBC) count in patients with B-cell chronic lymphocytic leukaemia (CLL).
Methods: Nonlinear mixed effects models were used to characterize plasma concentration-time data and WBC count-time data from 67 patients. Logistic regression was used to relate summary measures of drug exposure to tumour response.
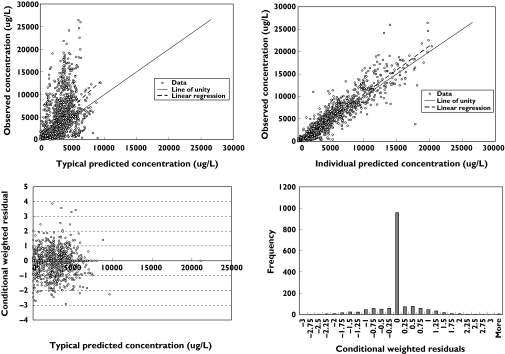
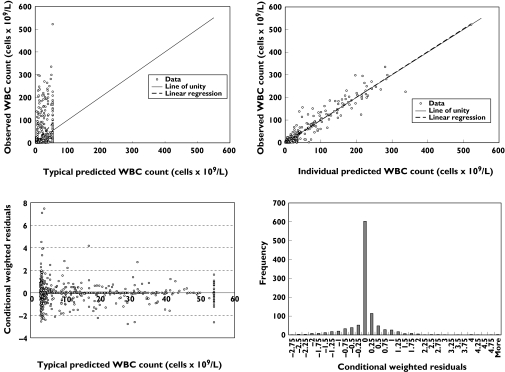
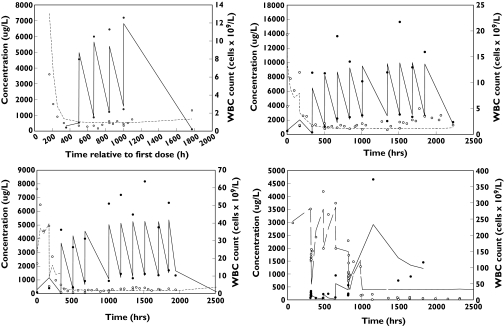
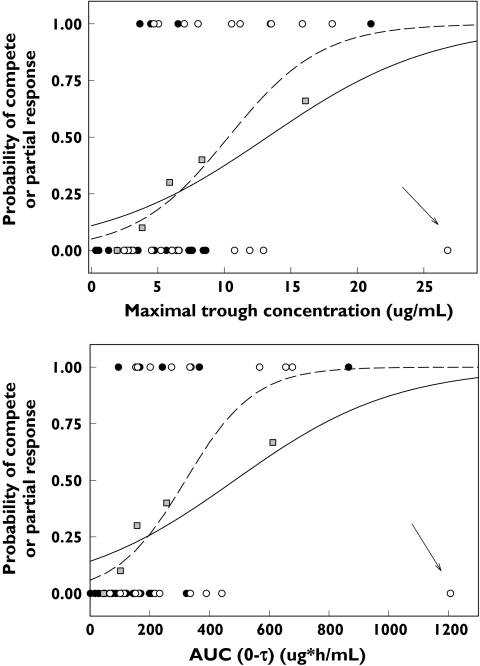
Results: Alemtuzumab pharmacokinetics were best characterized by a two-compartment model with nonlinear elimination where V(max) (microg h(-1)) was [1020 x (WBC count/10 x 10(9) l(-1))(0.194)], K(m) was 338 microg l(-1), V(1) was 11.3 l, Q was 1.05 l h(-1) and V(2) was 41.5 l. Intersubject variability (ISV) in V(max), K(m), V(1) and V(2) was 32%, 145%, 84% and 179%, respectively. The reduction in WBC over time was modelled by a stimulatory loss indirect response model with values of 18.2 for E(max), 306 microg l(-1) for EC(50), 1.56 x 10(9) cells l(-1) h(-1) for K(in) and 0.029 per h for K(out). The probability of achieving a complete or partial response was >/=50% when the maximal trough concentration exceeded 13.2 microg ml(-1) or when AUC(0-tau) exceeded 484 microg h(-1) ml(-1).
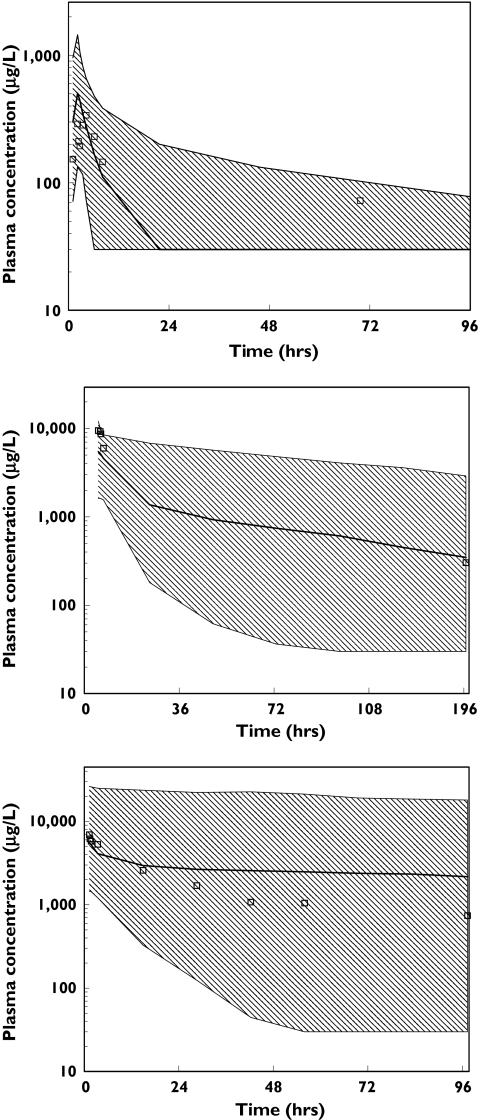
Conclusions: Alemtuzumab displayed time- and concentration-dependent pharmacokinetics with large interpatient variability, both in pharmacokinetics and pharmacodynamics, which was probably reflective of differences in tumour burden among patients. A direct relationship between maximal trough concentrations and clinical outcomes was observed, with increasing alemtuzumab exposure resulting in a greater probability of positive tumour response.
Figures
References
-
- Keating MJ, Flinn I, Jain V, Binet JL, Hillmen P, Byrd J, Albitar M, Brettman L, Santabarbara P, Wacker B, Rai KR. Therapeutic role of alemtuzumab (Campath-1H) in patients who have failed fludarabine: results of a large international study. Blood. 2002;99:3554–61. - PubMed
-
- Moreau T, Coles A, Wing M, Thorpe J, Miller D, Moseley I, Issacs J, Hale G, Clayton D, Scolding N, Waldmann H, Compston A. CAMPATH-IH in multiple sclerosis. Mult Sclerosis. 1996;1:357–65. - PubMed
-
- Knechtle SJ. Present experience with Campath-1H in organ transplantation and its potential use in pediatric recipients. Pediatr Tranplant. 2004;8:106–12. - PubMed
-
- Isaacs JD, Manna VK, Rapson N, Bulpitt KJ, Hazleman BL, Matteson EL, St Clair EW, Schnitzer TJ, Johnston JM. CAMPATH-1H in rheumatoid arthritis – an intravenous dose-ranging study. Br J Rheumatol. 1996;35:231–40. - PubMed
-
- Hale G, Rebello P, Brettman LR, Fegan C, Kennedy B, Kimby Leach M, Lundin J, Mellstedt H, Moreton P, Rawstron AC, Waldmann H, Osterberg A, Hillmen P. Blood concentrations of alemtuzumab and antiglobulin responses in patients with chronic lymphocytic leukemia following intravenous or subcutaneous routes of administration. Blood. 2004;104:948–55. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
