

Reducing one million child deaths from birth asphyxia--a survey of health systems gaps and priorities
- PMID: 17506872
- PMCID: PMC1888686
- DOI: 10.1186/1478-4505-5-4
Reducing one million child deaths from birth asphyxia--a survey of health systems gaps and priorities
Abstract
Background: Millions of child deaths and stillbirths are attributable to birth asphyxia, yet limited information is available to guide policy and practice, particularly at the community level. We surveyed selected policymakers, programme implementers and researchers to compile insights on policies, programmes, and research to reduce asphyxia-related deaths.
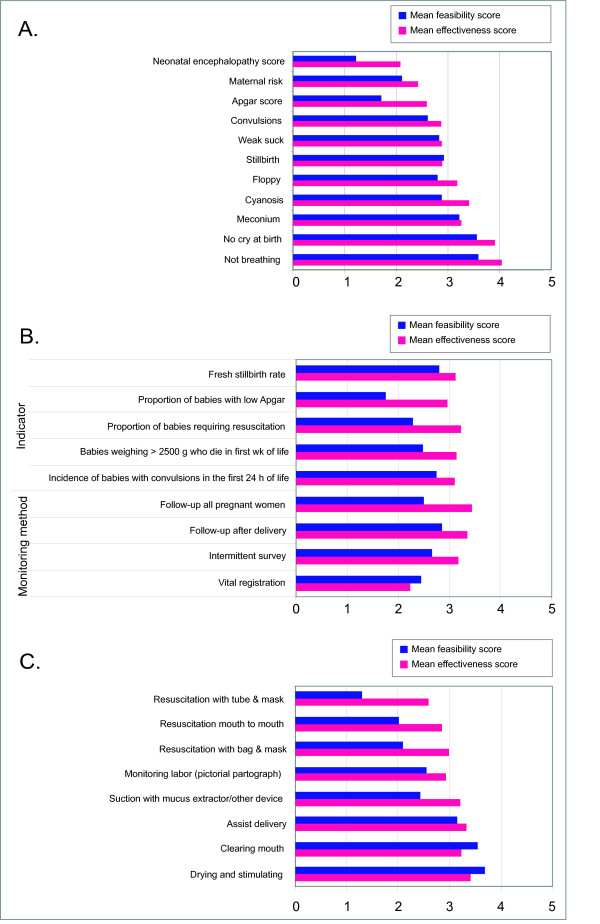
Method: A questionnaire was developed and pretested based on an extensive literature review, then sent by email (or airmail or fax, when necessary) to 453 policymakers, programme implementers, and researchers active in child health, particularly at the community level. The survey was available in French and English and employed 5-point scales for respondents to rate effectiveness and feasibility of interventions and indicators. Open-ended questions permitted respondents to furnish additional details based on their experience. Significance testing was carried out using chi-square, F-test and Fisher's exact probability tests as appropriate.
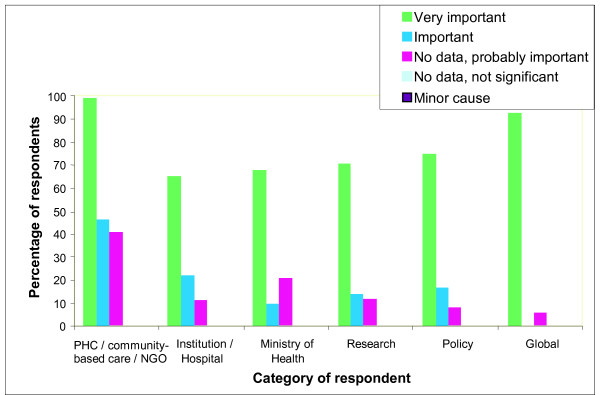
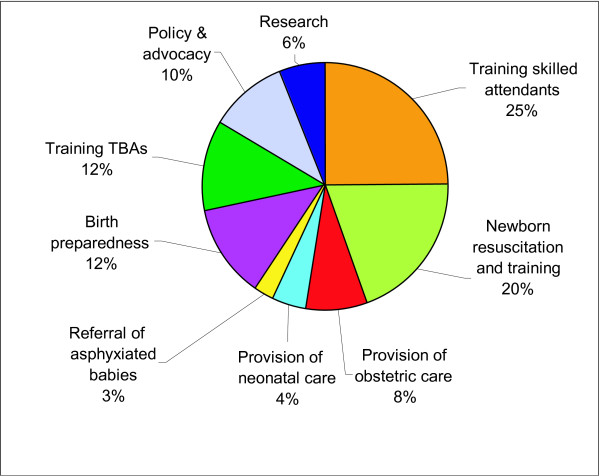
Results: 173 individuals from 32 countries responded (44%). National newborn survival policies were reported to exist in 20 of 27 (74%) developing countries represented, but respondents' answers were occasionally contradictory and revealed uncertainty about policy content, which may hinder policy implementation. Respondents emphasized confusing terminology and a lack of valid measurement indicators at community level as barriers to obtaining accurate data for decision making. Regarding interventions, birth preparedness and essential newborn care were considered both effective and feasible, while resuscitation at community level was considered less feasible. Respondents emphasized health systems strengthening for both supply and demand factors as programme priorities, particularly ensuring wide availability of skilled birth attendants, promotion of birth preparedness, and promotion of essential newborn care. Research priorities included operationalising birth preparedness, effectively evaluating pregnancy risk in the community, ensuring roles for traditional birth attendants (TBAs) that link them with the health system, testing the cost-effectiveness of various community cadres for resuscitation, and developing a clear case definition for case management and population monitoring.
Conclusion: Without more attention to improve care and advance birth asphyxia research, the 2 million deaths related to asphyxia, plus associated maternal deaths, will remain out of reach of effective care, either skilled or community level, for many years to come.
Figures
References
-
- Shibuya K, Murray C. Birth Asphyxia. In: Murray C and Lopez A, editor. The Global Burden of Disease: a comprehensive assessment of mortality and disability from diseases, injuries and risk factors in 1990 and projected to 2020. Cambridge, MA, Harvard University Press; 1996. pp. 429–453.
LinkOut - more resources
Full Text Sources
