

The effects of a glucose load and sympathetic challenge on autonomic function in obese women with and without type 2 diabetes mellitus
- PMID: 17512310
- PMCID: PMC1978097
- DOI: 10.1016/j.metabol.2007.02.001
The effects of a glucose load and sympathetic challenge on autonomic function in obese women with and without type 2 diabetes mellitus
Abstract
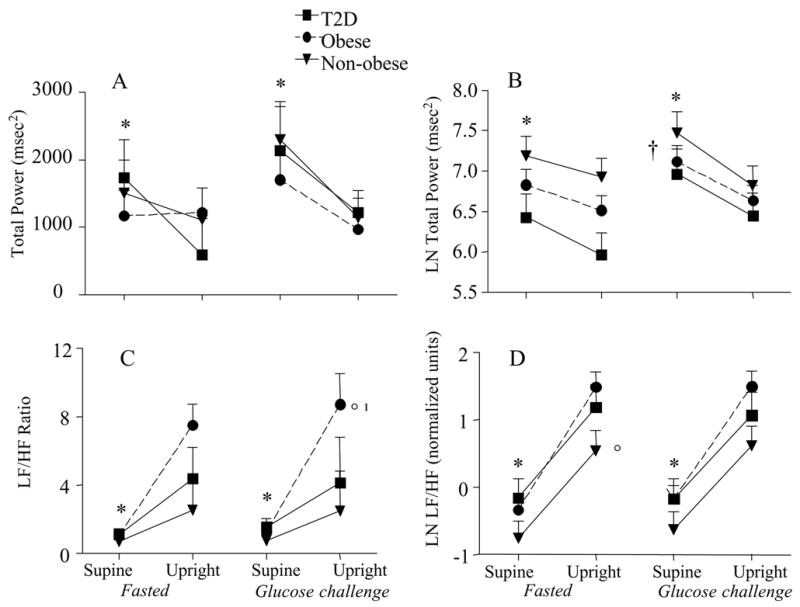
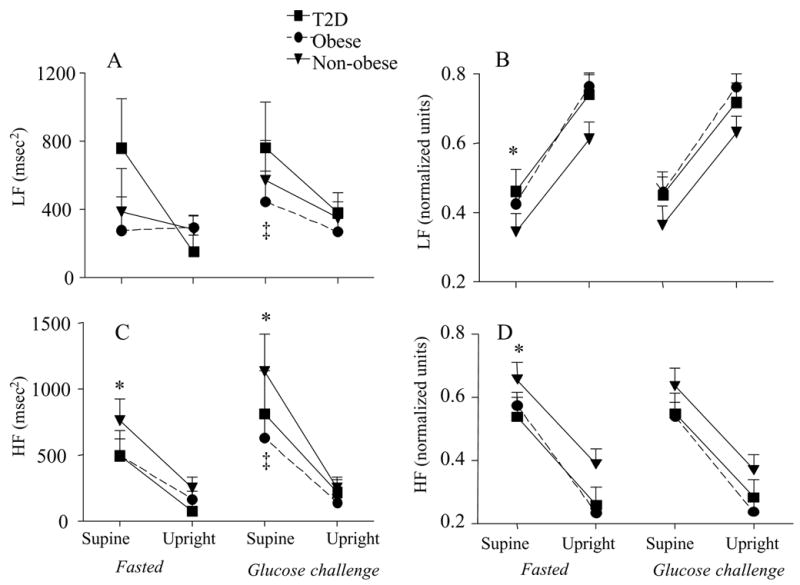
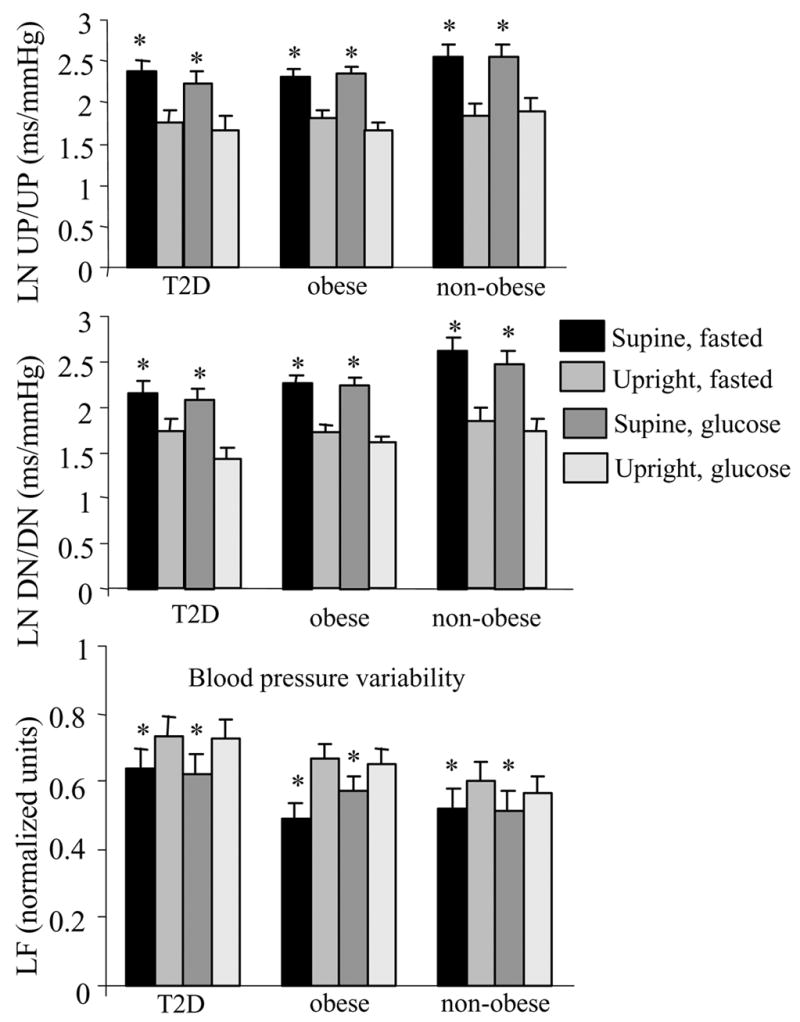
This study examined the effect of glucose ingestion on cardiac autonomic function in nonobese women and obese women with and without type 2 diabetes mellitus. Heart rate variability was measured via continuous electrocardiogram, and beat-by-beat blood pressure was recorded using finger photoplethysmography (Portapres, TNO Biomedical Instrumentation, Amsterdam, The Netherlands) in a fasted state and in response to a 75-g glucose load in 42 middle-aged women (40-60 years). Upright tilt was also used as an orthostatic stress to provide a clinically relevant challenge to the cardiovascular system. Significant main effects for log-transformed (Ln) total power (TP, square milliseconds) were observed with upright tilt (P < .01) and glucose challenge (P < .05). LnTP decreased in all groups in both the fasted and fed state with upright tilt (P < .01), but glucose ingestion resulted in higher LnTP in the supine position only (P = .008). Tilt resulted in a significant main effect for low-frequency (LFnu, calculated in normalized units) and high-frequency (HFnu, calculated in normalized units) power (P < .000), whereas the glucose challenge had no effect on LFnu or HFnu power. LFnu approached significance for group differences (P = .07), such that the nonobese had lower LF power than either of the obese groups. Sympathovagal balance (LnLF/HF ratio) was affected by position (P < .000) and group (P < .05), with a lower LnLF/HF in the nonobese than in the obese women. Baroreceptor sensitivity decreased (P < .01) during upright tilt but was not changed by the glucose challenge. In conclusion, basal sympathovagal balance is higher in obese individuals with and without type 2 diabetes mellitus. Women with type 2 diabetes mellitus showed no differences in autonomic function with an orthostatic challenge or glucose load than nondiabetic, obese women. The glucose load did alter total spectral power in all of these middle-aged women but had no impact on baroreceptor sensitivity.
Figures
References
-
- Ewing D, Campbell I, Clarke B. The natural history of diabetic autonomic neruopathy. Q J Med. 1980;49:95–108. - PubMed
-
- Gottsater A, Ahmed M, Fernlund P, Sundkvist G. Autonomic neuropathy in Type 2 diabetic patients is associated with hyperinsulinaemia and hypertriglyceridaemia. Diabet Med. 1999;16:49–54. - PubMed
-
- Emdin M, Gastaldelli A, Muscelli E, et al. Hyperinsulinemia and autonomic nervous system dysfunction in obesity: effects of weight loss. Circulation. 2001;103:513–519. - PubMed
-
- Muscelli E, Emdin M, Natali A, et al. Autonomic and hemodynamic responses to insulin in lean and obese humans. J Clin Endocrinol Metab. 1998;83:2084–2090. - PubMed
-
- Piccirillo G, Vetta F, Fimognari FL, et al. Power spectral analysis of heart rate variability in obese subjects: evidence of decreased cardiac sympathetic responsiveness. Int J Obes Relat Metab Disord. 1996;20:825–829. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
