

Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy
- PMID: 17513807
- PMCID: PMC2670394
- DOI: 10.1200/JCO.2006.08.9607
Predicting the outcome of salvage radiation therapy for recurrent prostate cancer after radical prostatectomy
Erratum in
- J Clin Oncol. 2007 Sep 10;25(26):4153
Abstract
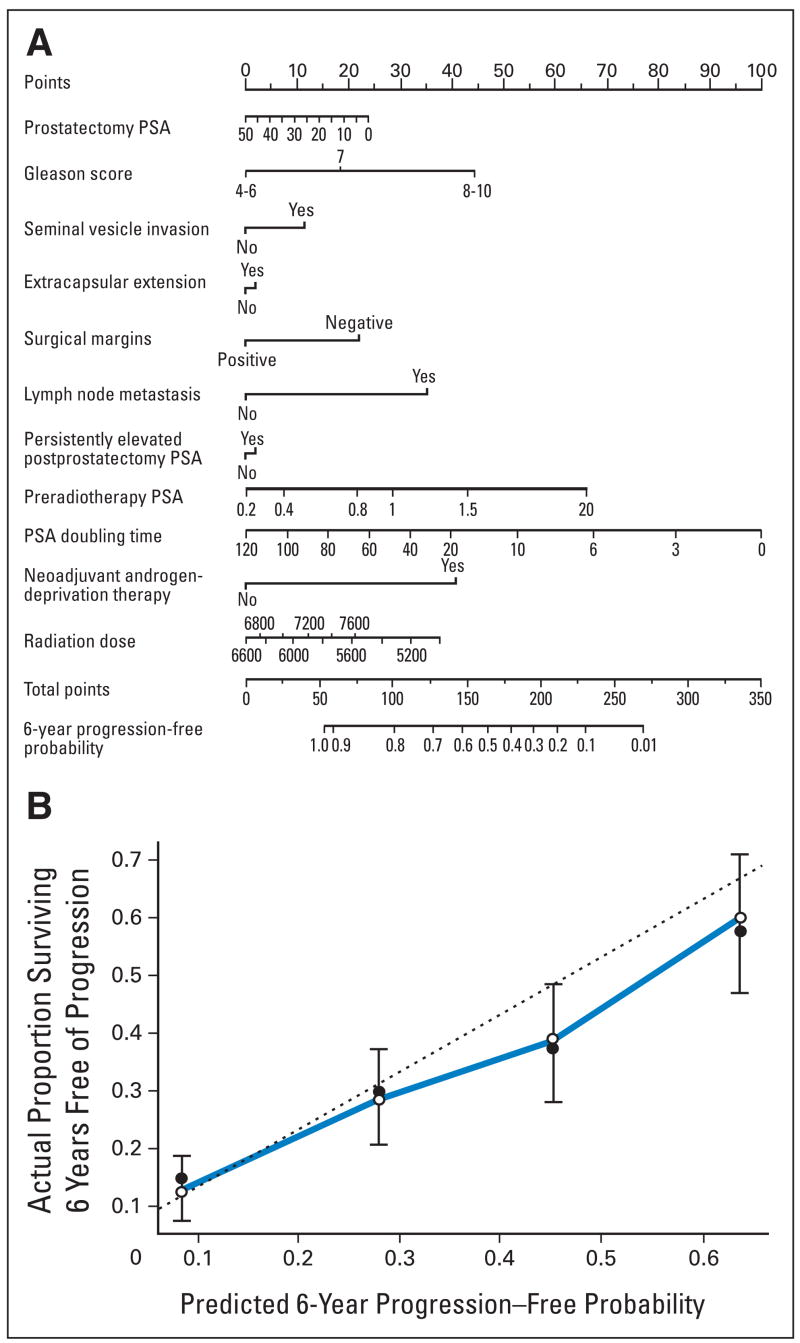
Purpose: An increasing serum prostate-specific antigen (PSA) level is the initial sign of recurrent prostate cancer among patients treated with radical prostatectomy. Salvage radiation therapy (SRT) may eradicate locally recurrent cancer, but studies to distinguish local from systemic recurrence lack adequate sensitivity and specificity. We developed a nomogram to predict the probability of cancer control at 6 years after SRT for PSA-defined recurrence.
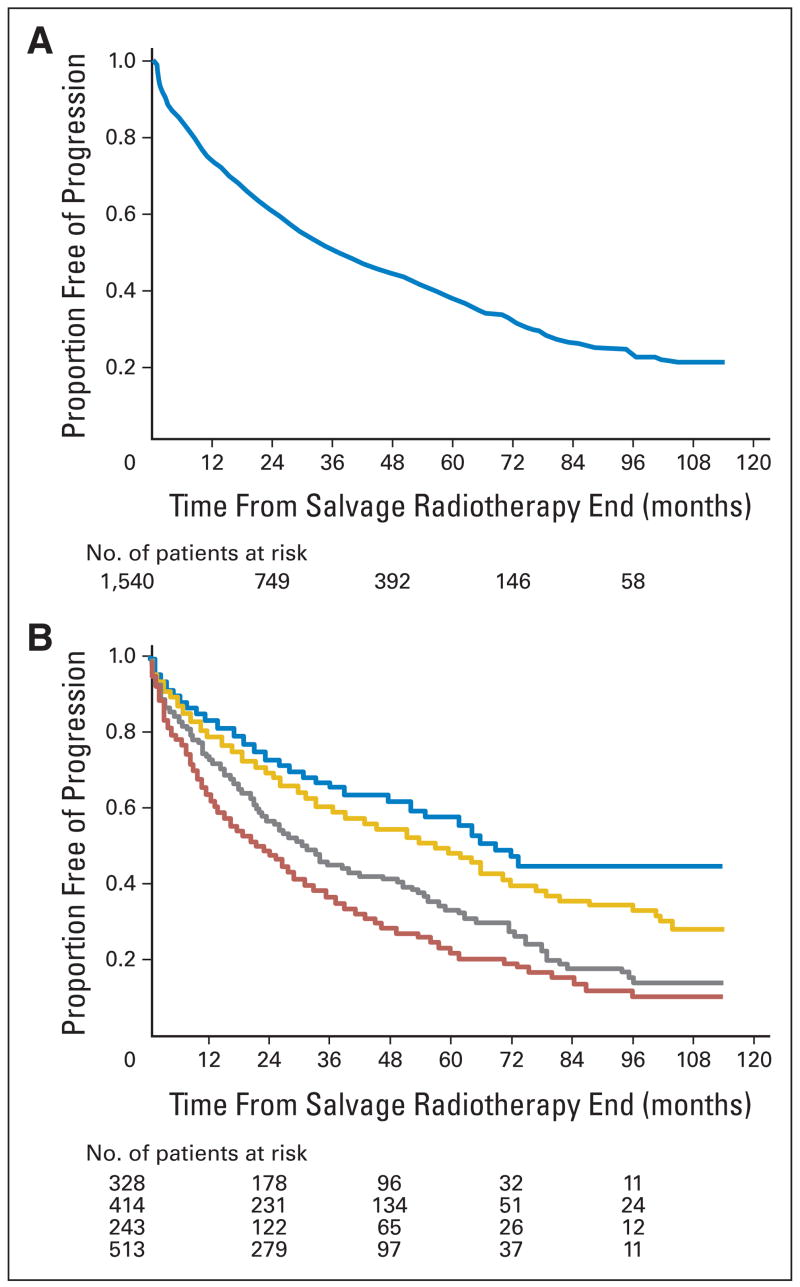
Patients and methods: Using multivariable Cox regression analysis, we constructed a model to predict the probability of disease progression after SRT in a multi-institutional cohort of 1,540 patients.
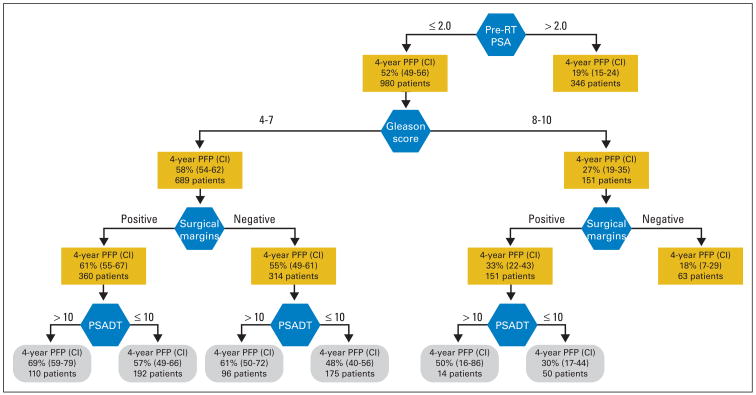
Results: The 6-year progression-free probability was 32% (95% CI, 28% to 35%) overall. Forty-eight percent (95% CI, 40% to 56%) of patients treated with SRT alone at PSA levels of 0.50 ng/mL or lower were disease free at 6 years, including 41% (95% CI, 31% to 51%) who also had a PSA doubling time of 10 months or less or poorly differentiated (Gleason grade 8 to 10) cancer. Significant variables in the model were PSA level before SRT (P < .001), prostatectomy Gleason grade (P < .001), PSA doubling time (P < .001), surgical margins (P < .001), androgen-deprivation therapy before or during SRT (P < .001), and lymph node metastasis (P = .019). The resultant nomogram was internally validated and had a concordance index of 0.69.
Conclusion: Nearly half of patients with recurrent prostate cancer after radical prostatectomy have a long-term PSA response to SRT when treatment is administered at the earliest sign of recurrence. The nomogram we developed predicts the outcome of SRT and should prove valuable for medical decision making for patients with a rising PSA level.
Conflict of interest statement
Authors’ disclosures of potential conflicts of interest and author contributions are found at the end of this article.
AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST
Although all authors completed the disclosure declaration, the following authors or their immediate family members indicated a financial interest. No conflict exists for drugs or devices used in a study if they are not being evaluated as part of the investigation. For a detailed description of the disclosure categories, or for more information about ASCO’s conflict of interest policy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section in Information for Contributors.
Figures
References
-
- Bianco FJ, Jr, Scardino PT, Eastham JA. Radical prostatectomy: Long-term cancer control and recovery of sexual and urinary function (“trifecta”) Urology. 2005;66:83–94. - PubMed
-
- Pound CR, Partin AW, Eisenberger MA, et al. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999;281:1591–1597. - PubMed
-
- Anscher MS, Clough R, Dodge R. Radiotherapy for a rising prostate-specific antigen after radical prostatectomy: The first 10 years. Int J Radiat Oncol Biol Phys. 2000;48:369–375. - PubMed
-
- Catton C, Gospodarowicz M, Warde P, et al. Adjuvant and salvage radiation therapy after radical prostatectomy for adenocarcinoma of the prostate. Radiother Oncol. 2001;59:51–60. - PubMed
-
- Cheung R, Kamat AM, de Crevoisier R, et al. Outcome of salvage radiotherapy for biochemical failure after radical prostatectomy with or without hormonal therapy. Int J Radiat Oncol Biol Phys. 2005;63:134–140. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
