

Frequency of adverse events in patients with poor anticoagulation: a meta-analysis
- PMID: 17515585
- PMCID: PMC1867836
- DOI: 10.1503/cmaj.061523
Frequency of adverse events in patients with poor anticoagulation: a meta-analysis
Erratum in
- CMAJ. 2007 Jul 31;177(3):271
Abstract
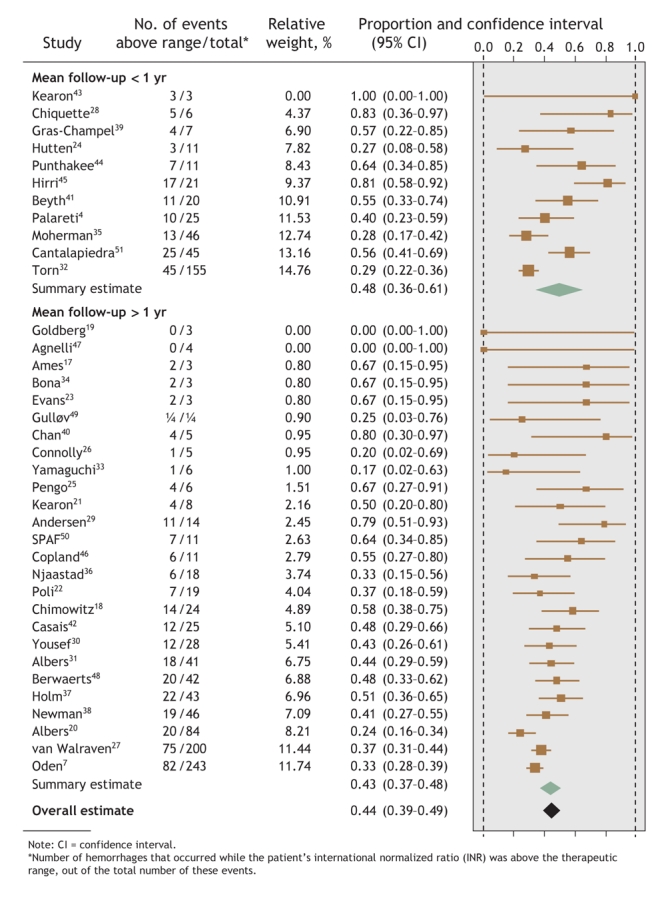
Background: Patients taking anticoagulants orally over the long term have international normalized ratios (INRs) outside the individual therapeutic range more than one-third of the time. Improved anticoagulation control will reduce hemorrhagic and thromboembolic event rates. To gauge the potential effect of improved anticoagulation control, we undertook to determine the proportion of anticoagulant-associated events that occur when INRs are outside the therapeutic range.
Methods: We conducted a meta-analysis of all studies that assigned hemorrhagic and thromboembolic events in patients taking anticoagulants to discrete INR ranges. We identified studies using the MEDLINE (1966-2006) and EMBASE (1980-2006) databases. We included studies reported in English if the majority of patients taking oral anticoagulants had an INR range with a lower limit between 1.8 and 2 and an upper limit between 3 and 3.5, and their INR at the time of the hemorrhagic or thromboembolic event was recorded.
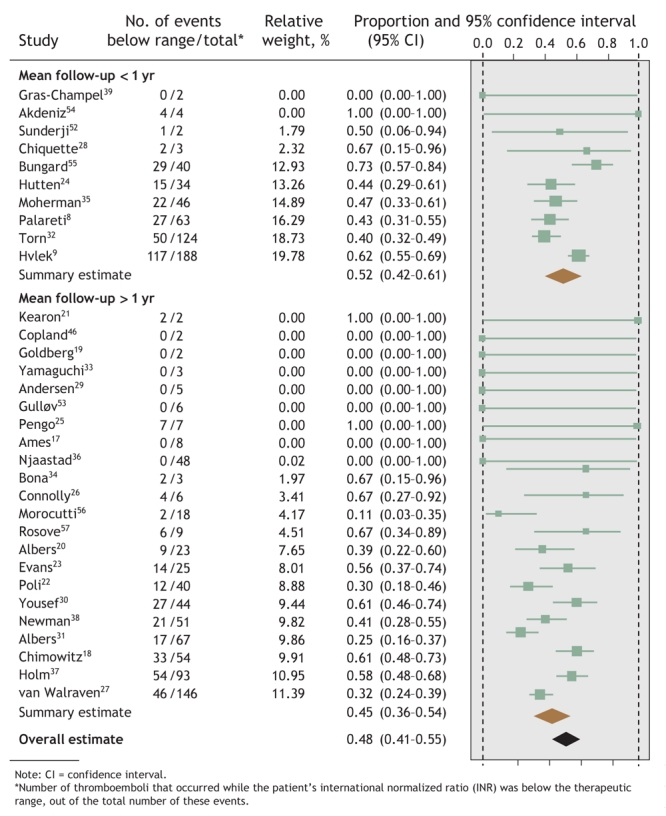
Results: The final analysis included results from 45 studies (23 that reported both hemorrhages and thromboemboli; 14 that reported hemorrhages only; and 8, thromboemboli only) involving a median of 208 patients (limits of interquartile range [25th-75th percentile] 131-523 subjects; total n = 71 065). Of these studies, 64% were conducted at community practices; the remainder, at anticoagulation clinics. About 69% of the studies were classed as having moderate or high quality. Overall, 44% (95% confidence interval [CI] 39%-49%) of hemorrhages occurred when INRs were above the therapeutic range, and 48% (95% CI 41%-55%) of thromboemboli took place when below it. The mean proportion of events that occurred while the patient's INR was outside the therapeutic range was greater for studies with a short mean follow-up (< 1 yr). Between-study heterogeneity was significant (p < 0.001).
Interpretation: Improved anticoagulation control could decrease the likelihood of almost half of all anticoagulant-associated adverse events.
Figures
Comment in
-
Genetic analysis to prevent warfarin complications.CMAJ. 2007 Aug 14;177(4):377. doi: 10.1503/cmaj.1070081. CMAJ. 2007. PMID: 17698833 Free PMC article. No abstract available.
References
-
- van Walraven C, Jennings A, Oake N, et al. Effect of study setting on anticoagulation control: a systematic review and metaregression. Chest 2006;129:1155-66. - PubMed
-
- Veeger NJGM, Piersma-Wichers M, Hillege HL, et al. Early detection of patients with a poor response to vitamin K antagonists: the clinical impact of individual time within target range in patients with heart disease. J Thromb Haemost 2006;4:1625-7. - PubMed
-
- Veeger NJGM, Piersma-Wichers M, Tijssen JG, et al. Individual time within target range in patients treated with vitamin K antagonists: main determinant of quality of anticoagulation and predictor of clinical outcome. A retrospective study of 2300 consecutive patients with venous thromboembolism. Br J Haematol 2005;128:513-9. - PubMed
-
- Palareti G, Leali N, Coccheri S, et al. Bleeding complications of oral anticoagulant treatment: an inception-cohort, prospective collaborative study (ISCOAT). Italian Study on Complications of Oral Anticoagulant Therapy. Lancet 1996;348:423-8. - PubMed
-
- Torn M, Algra A, Rosendaal FR. Oral anticoagulation for cerebral ischemia of arterial origin: high initial bleeding risk. Neurology 2001;57:1993-9. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical