

Factor XIIIA-V34L and factor XIIIB-H95R gene variants: effects on survival in myocardial infarction patients
- PMID: 17515963
- PMCID: PMC1869629
- DOI: 10.2119/2006-00049.Gemmati
Factor XIIIA-V34L and factor XIIIB-H95R gene variants: effects on survival in myocardial infarction patients
Abstract
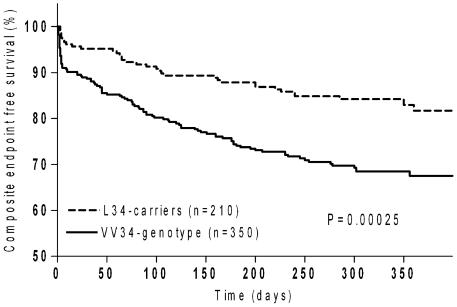
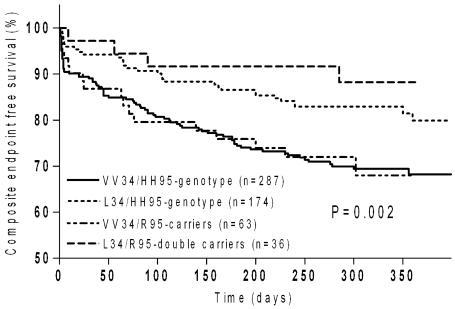
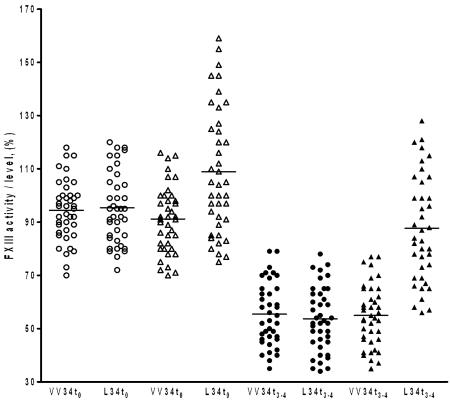
It has been demonstrated recently that coagulation factor XIII (FXIII) plays an extraordinary role in myocardial healing after infarction, improving survival in a mouse model. Common FXIII gene variants (i.e. FXIIIA-V34L and FXIIIB-H95R) significantly influence the molecular activity. To evaluate whether there is a relationship between the two FXIII gene variants and survival in patients after myocardial infarction (MI), V34L and H95R were PCR-genotyped in a cohort of 560 MI cases and follow-up was monitored. Cases with ST-segment elevation MI (STEMI) were 416 (74.3%) and 374 of these were treated with primary percutaneous coronary intervention (PCI) (89.9%). The remaining 144 patients showed non-ST-segment elevation MI (NSTEMI) at enrollment. The combined endpoint was the occurrence of death, re-infarction, and heart failure. Kaplan-Meier analysis at one year yielded an overall rate for adverse events of 24.5% with a lower incidence in the L34-carriers (28.8% vs 17.1%; log-rank, P = 0.00025), similar to that of the 416 STEMI (23.8%) being (28.0% and 16.9%; VV34- and L34-carriers respectively; log-rank, P = 0.001). Primary PCI-group had a slight lower incidence (22.9%) of adverse events (26.8% and 17.1%; VV34- and L34-carriers respectively; log-rank, P = 0.009). During hospitalization, 506 patients received PCI (374 primary PCI and 132 elective PCI). Significance was conserved also in the overall PCI-group (28.6% and 17.8%; VV34- and L34-carriers respectively; log-rank, P = 0.001). Similar findings were observed at 30 days follow-up. Cases carrying both FXIII variants had improved survival rate (log-rank, P = 0.019). On the other hand, minor bleeding complications were found increased in L34-carriers (P = 0.0001) whereas major bleeding complications were not. Finally, more direct evidence on the role of FXIII molecule on survival might come from the fact that despite significant FXIII antigen reductions observed in cases after MI, regardless the FXIII genotype considered, L34-carriers kept almost normal FXIII activity (VV34- vs L34-carriers; P < 0.001). We conclude that FXIII L34-allele improves survival after MI in all the groups analyzed, possibly through its higher activity associated with assumable positive effects on myocardial healing and recovered functions. Genetically determined higher FXIII activity might influence post-MI outcome. This paves the way for using FXIII molecules to improve myocardial healing, recovery of functions, and survival after infarction.
Figures
References
-
- Dardik R, et al. Evaluation of the pro-angiogenic effect of factor XIII in heterotopic mouse heart allografts and FXIII-deficient mice. Thromb Haemost. 2006;95:546–50. - PubMed
-
- Dardik R, et al. Novel proangiogenic effect of factor XIII associated with suppression of thrombospondin 1 expression. Arterioscler Thromb Vasc Biol. 2003;23:1472–7. - PubMed
-
- Dardik R, Loscalzo J, Inbal A. Factor XIII (FXIII) and angiogenesis. J Thromb Haemost. 2006;1:19–25. - PubMed
-
- Herouy Y, Hellstern MO, Vanscheidt W, Schopf E, Norgauer J. Factor XIII-mediated inhibition of fibrinolysis and venous leg ulcers. Lancet. 2000;355:1970–1. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous