

Clinical trial of autologous formalin-fixed tumor vaccine for glioblastoma multiforme patients
- PMID: 17517052
- PMCID: PMC11158799
- DOI: 10.1111/j.1349-7006.2007.00518.x
Clinical trial of autologous formalin-fixed tumor vaccine for glioblastoma multiforme patients
Abstract
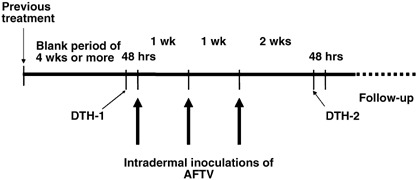
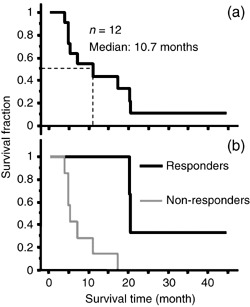
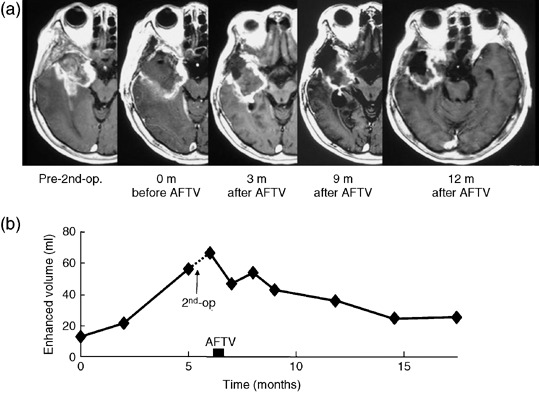
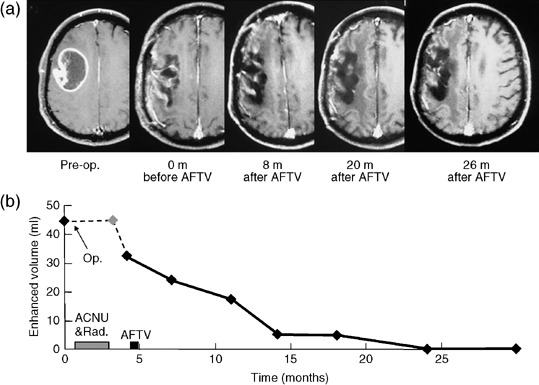
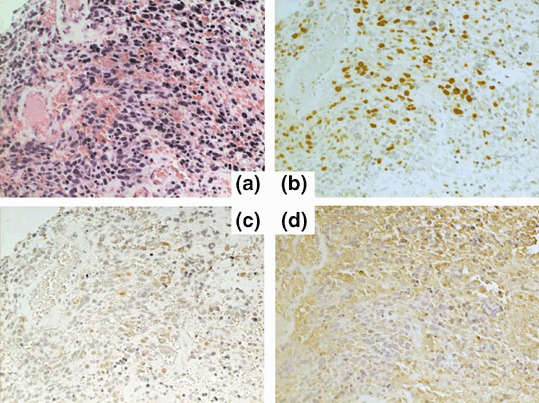
A pilot study was performed to investigate the safety and feasibility of autologous formalin-fixed tumor vaccines (AFTV) and the clinical responses to these vaccines by glioblastoma multiforme (GBM) patients. Twelve primary GBM patients were recruited. Eight had recurrent disease while four had been treated for primary disease but retained a visible tumor mass. AFTV were prepared from formalin-fixed and/or paraffin-embedded tumor tissue obtained upon surgery and premixed with original adjuvant materials. The patients were given three five-site intradermal inoculations at weekly intervals. A delayed-type hypersensitivity test was performed before and after each vaccination. In addition, the tumor tissues were subjected to immunohistochemical analysis to determine whether MIB-1, p53, and major histocompatibility complex (MHC) class-I complex expression could predict the response to the treatment. The treatment was well tolerated, with only local erythema, induration, and low-grade fever being reported. Of the 12 patients, one showed a complete response, one showed a partial response, two showed minor responses, one had stable disease, and seven exhibited progressive disease. The median survival period was 10.7 months from the initiation of the AFTV treatment but three of the five responders survived for 20 months or more after AFTV inoculation. Low p53 and high MHC class-I expression by the tumor may help predict the efficacy of this therapy. Thus, the AFTV is safe and feasible, and could significantly improve the outcome of GBM. Further clinical investigations to confirm this are highly desirable.
Figures
References
-
- The Committee of Brain Tumor Registry of Japan . Report of Brain Tumor Registry of Japan (1969–96), 11th edn. Neurolgia Medico‐Chirurugica, 43 (Suppl.). Tokyo: The Japan Neurological Society, 2003.
-
- Hulshof MC, Koot RW, Schimmel EC et al . Prognostic factors in glioblastoma multiforme. 10 years experience of a single institution. Strahlenther Onkol 2001; 177: 283–90. - PubMed
-
- Lacroix M, Abi‐Said D, Fourney DR et al . A multivariate analysis of 416 patients with glioblastoma multiforme: prognosis, extent of resection, and survival. J Neurosurg 2001; 95: 190–8. - PubMed
-
- Prados MD, Larson DA, Lamborn K et al . Radiation therapy and hydroxyurea followed by the combination of 6‐thioguanine and BCNU for the treatment of primary malignant brain tumors. Int J Radiat Oncol Biol Phys 1998; 40: 57–63. - PubMed
-
- Shrieve DC, Alexander E III, Black PM et al . Treatment of patients with primary glioblastoma multiforme with standard postoperative radiotherapy and radiosurgical boost: prognostic factors and long‐term outcome. J Neurosurg 1999; 90: 72–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
