

Rosiglitazone RECORD study: glucose control outcomes at 18 months
- PMID: 17517066
- PMCID: PMC1974811
- DOI: 10.1111/j.1464-5491.2007.02160.x
Rosiglitazone RECORD study: glucose control outcomes at 18 months
Abstract
Aims: To compare glucose control over 18 months between rosiglitazone oral combination therapy and combination metformin and sulphonylurea in people with Type 2 diabetes.
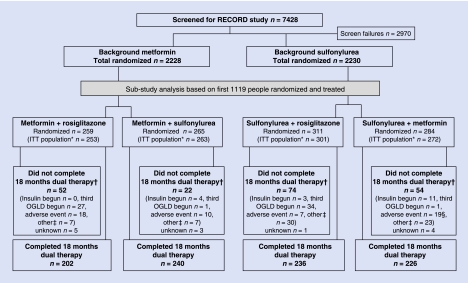
Methods: RECORD, a multicentre, parallel-group study of cardiovascular outcomes, enrolled people with an HbA(1c) of 7.1-9.0% on maximum doses of metformin or sulphonylurea. If on metformin they were randomized to add-on rosiglitazone or sulphonylurea (open label) and if on sulphonylurea to rosiglitazone or metformin. HbA(1c) was managed to < or = 7.0% by dose titration. A prospectively defined analysis of glycaemic control on the first 1122 participants is reported here, with a primary outcome assessed against a non-inferiority margin for HbA(1c) of 0.4%.
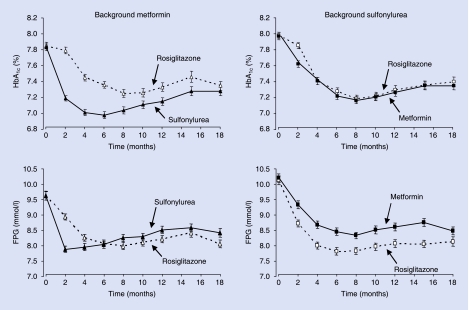
Results: At 18 months, HbA(1c) reduction on background metformin was similar with rosiglitazone and sulphonylurea [difference 0.07 (95% CI -0.09, 0.23)%], as was the change when rosiglitazone or metformin was added to sulphonylurea [0.06 (-0.09, 0.20)%]. At 6 months, the effect on HbA(1c) was greater with add-on sulphonylurea, but was similar whether sulphonylurea was added to rosiglitazone or metformin. Differences in fasting plasma glucose were not statistically significant at 18 months [rosiglitazone vs. sulphonylurea -0.36 (-0.74, 0.02) mmol/l, rosiglitazone vs. metformin -0.34 (-0.73, 0.05) mmol/l]. Increased homeostasis model assessment insulin sensitivity and reduced C-reactive protein were greater with rosiglitazone than metformin or sulphonylurea (all P < or = 0.001). Body weight was significantly increased with rosiglitazone compared with sulphonylurea [difference 1.2 (0.4, 2.0) kg, P = 0.003] and metformin [difference 4.3 (3.6, 5.1) kg, P < 0.001].
Conclusions: In people with diabetes, rosiglitazone in combination with metformin or sulphonylurea was demonstrated to be non-inferior to the standard combination of metformin + sulphonylurea in lowering HbA(1c) over 18 months, and produces greater improvements in C-reactive protein and basal insulin sensitivity but is also associated with greater weight gain.
Figures
References
-
- IDF Clinical Guidelines Task Force. Global guideline for Type 2 diabetes: recommendations for standard, comprehensive and minimal care. Diabet Med. 2006;23:579–593. - PubMed
-
- Matthews DR, Cull CA, Stratton IM, Holman RR, Turner RC. Sulphonylurea failure in non-insulin-dependent diabetic patients over 6 years (UKPDS 26) Diabet Med. 1998;15:297–303. - PubMed
-
- UK Prospective Diabetes Study (UKPDS) Group. Intensive blood-glucose control with sulphonylureas or insulin compared with conventional treatment and risk of complications in patients with type 2 diabetes (UKPDS 33) Lancet. 1998;352:837–853. - PubMed
-
- Turner RC, Cull CA, Frighi V, Holman RR. Glycaemic control with diet, sulphonylurea, metformin, or insulin in patients with Type 2 diabetes mellitus: progressive requirement for multiple therapies (UKPDS 49) J Am Med Assoc. 1999;281:2005–2012. - PubMed
-
- Burke JP, Williams K, Gaskill SP, Hazuda HP, Haffner SM, Stern MP. Rapid rise in the incidence of type 2 diabetes from 1987 to 1996: results from the San Antonio Heart Study. Arch Int Med. 1999;159:1450–1456. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
