

Can asthma control be improved by understanding the patient's perspective?
- PMID: 17518999
- PMCID: PMC1894634
- DOI: 10.1186/1471-2466-7-8
Can asthma control be improved by understanding the patient's perspective?
Abstract
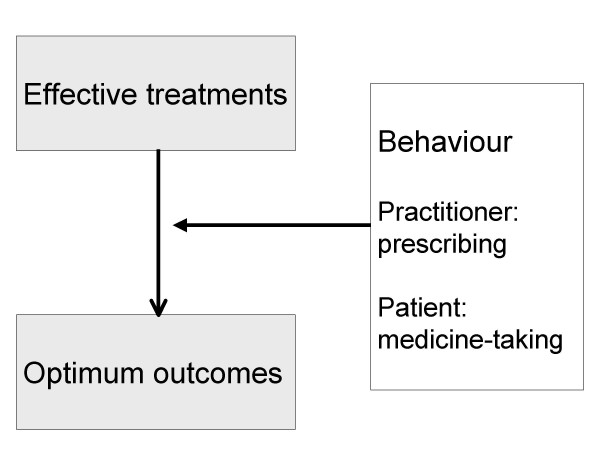
Background: Clinical trials show that asthma can be controlled in the majority of patients, but poorly controlled asthma still imposes a considerable burden. The level of asthma control achieved reflects the behaviour of both healthcare professionals and patients. A key challenge for healthcare professionals is to help patients to engage in self-management behaviours with optimal adherence to appropriate treatment. These issues are particularly relevant in primary care, where most asthma is managed. An international panel of experts invited by the International Primary Care Respiratory Group considered the evidence and discussed the implications for primary care practice.
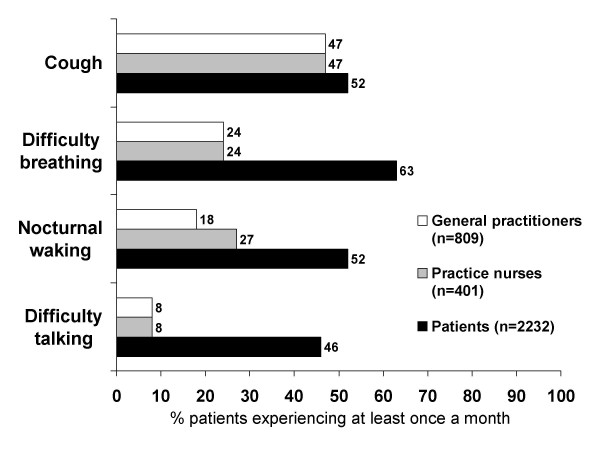
Discussion: Causes of poor control: Clinical factors such as exposure to triggers and concomitant rhinitis are important but so are patient behavioural factors. Behaviours such as smoking and nonadherence may reduce the efficacy of treatment and patients' perceptions influence these behaviours. Perceptual barriers to adherence include doubting the need for treatment when symptoms are absent and concerns about potential adverse effects. Under-treatment may also be related to patients' underestimation of the significance of symptoms, and lack of awareness of achievable control.
Implications: Three key implications for healthcare professionals emerged from the debate. First, the need for simple tools to assess asthma control. Two approaches considered were the monitoring of biometric markers of control and questionnaires to record patient-reported outcomes. Second, to understand the reasons for poor control for individual patients, identifying both clinical (e.g. rhinitis) and behavioural factors (e.g. smoking and nonadherence to treatment). Third was the need to incorporate, within asthma review, an assessment of patient perspectives including their goals and aspirations and to elicit their beliefs and concerns about asthma and its treatment. This can be used as a basis for agreement between the healthcare professional and patient on a predefined target regarding asthma control and a treatment plan to achieve this.
Summary: Optimum review of asthma is essential to improve control. A key priority is the development of simple and effective tools for identifying poor control for individual patients coupled with a tailored approach to treatment to enable patients to set and achieve realistic goals for asthma control.
Figures
References
-
- Global Initiative for Asthma (GINA) GINA http://www.ginasthma.com
-
- BTS British Thoracic Society/Scottish Intercollegiate Guidelines Network Guidelines on asthma management. Thorax. 2003;58:i1–i94. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
