

Haemoglobin and haematocrit: is the threefold conversion valid for assessing anaemia in malaria-endemic settings?
- PMID: 17519019
- PMCID: PMC1885442
- DOI: 10.1186/1475-2875-6-67
Haemoglobin and haematocrit: is the threefold conversion valid for assessing anaemia in malaria-endemic settings?
Abstract
Background: Anaemic status is determined by haemoglobin using the HemoCue system or haematocrit measurements, and a threefold conversion is commonly used to equate the two measures (haemoglobin = haematocrit/3). The validity of this conversion in malaria endemic settings was assessed.
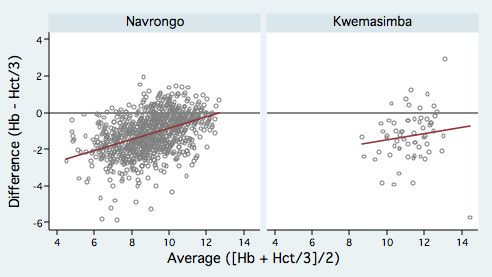
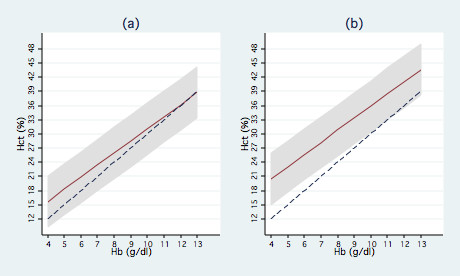
Methods: Concurrent measures of haemoglobin and centrifuged haematocrit in children aged 6-59 months were compared by modelling the difference between the two measures against their average. A random effects linear regression of the difference of the measures on their average was used to describe the line of best agreement and 95% limits of agreement for these two measures over a range of values after adjusting for statistically significant covariates.
Results: There was a consistent bias between the two measures, with haemoglobin less than haematocrit/3 in 87% (899/1,030) of observations. This difference was non-uniform, decreasing with the average measure, i.e. less difference at higher haemoglobin and haematocrit values. In these studies, use of haematocrit would have underestimated the prevalence of anaemia by misclassifying 10% (89/920) of individuals with haemoglobin < 11 g/dl, 66% (252/380) of individuals with haemoglobin < 8 g/dl and 100% (23/23) of individuals with haemoglobin < 5 g/dl. The mean difference between the measures was greater in males than females, increased with age between 6-59 months, and was greater in the wet than dry season suggesting that the relationship between haemoglobin and haematocrit may be modified by exposure to malaria.
Conclusion: The regression model indicated that the standard threefold conversion from haematocrit to haemoglobin underestimates the prevalence of haemoglobin < 11 g/dl in children under five years of age in malaria endemic settings. This bias was more acute for more severe anaemia defined by haemoglobin < 8 g/dl and haemoglobin < 5 g/dl. This has important implications for the comparability of studies using these different measures. Direct determination of haemoglobin should be the measurement of choice for assessing anaemia outcomes in malaria intervention trials and surveys.
Figures
References
-
- Chandramohan D, Owusu-Agyei S, Carneiro I, Awine T, Amponsa-Achiano K, Mensah N, Jaffar S, Baiden R, Hodgson A, Binka F, Greenwood B. Cluster randomised trial of intermittent preventive treatment for malaria in infants in area of high, seasonal transmission in Ghana. BMJ. 2005;331:727–733. doi: 10.1136/bmj.331.7519.727. - DOI - PMC - PubMed
-
- Curtis CF, Maxwell CA, Finch RJ, Njunwa KJ. A comparison of use of a pyrethroid either for house spraying or for bednet treatment against malaria vectors. Trop Med Int Health. 1998;3:619–631. - PubMed
-
- Menendez C, Kahigwa E, Hirt R, Vounatsou P, Aponte JJ, Font F, Acosta CJ, Schellenberg DM, Galindo CM, Kimario J, Urassa H, Brabin B, Smith TA, Kitua AY, Tanner M, Alonso PL. Randomised placebo-controlled trial of iron supplementation and malaria chemoprophylaxis for prevention of severe anaemia and malaria in Tanzanian infants. Lancet. 1997;350:844–850. doi: 10.1016/S0140-6736(97)04229-3. - DOI - PubMed
-
- Schellenberg D, Menendez C, Kahigwa E, Aponte J, Vidal J, Tanner M, Mshinda H, Alonso P. Intermittent treatment for malaria and anaemia control at time of routine vaccinations in Tanzanian infants: a randomised, placebo-controlled trial. Lancet. 2001;357:1471–1477. doi: 10.1016/S0140-6736(00)04643-2. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
