

Quantifying HIV-1 transmission due to contaminated injections
- PMID: 17522260
- PMCID: PMC1887593
- DOI: 10.1073/pnas.0610435104
Quantifying HIV-1 transmission due to contaminated injections
Abstract
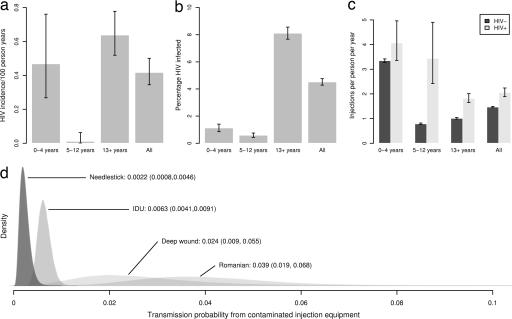
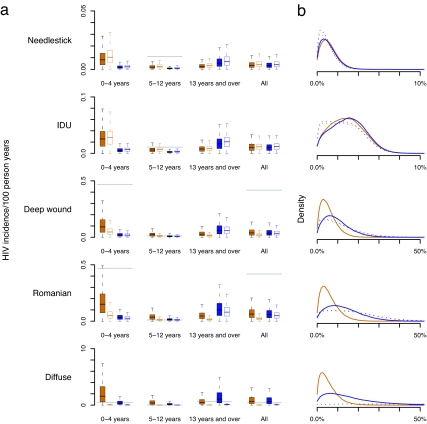
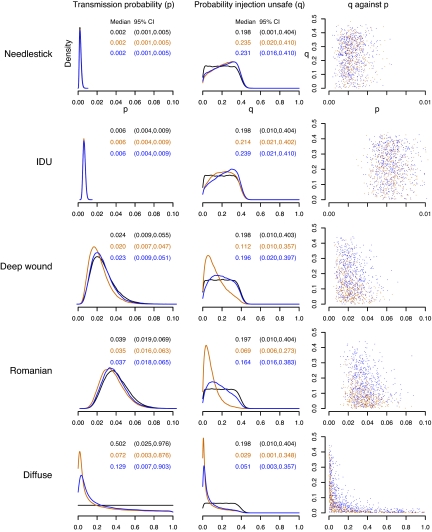
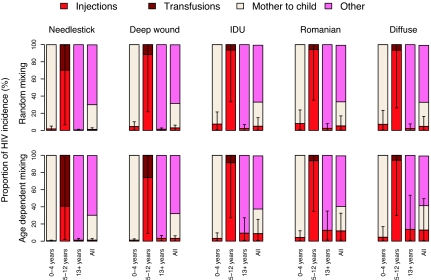
Assessments of the importance of different routes of HIV-1 (HIV) transmission are vital for prioritization of control efforts. Lack of consistent direct data and large uncertainty in the risk of HIV transmission from HIV-contaminated injections has made quantifying the proportion of transmission caused by contaminated injections in sub-Saharan Africa difficult and unavoidably subjective. Depending on the risk assumed, estimates have ranged from 2.5% to 30% or more. We present a method based on an age-structured transmission model that allows the relative contribution of HIV-contaminated injections, and other routes of HIV transmission, to be robustly estimated, both fully quantifying and substantially reducing the associated uncertainty. To do this, we adopt a Bayesian perspective, and show how prior beliefs regarding the safety of injections and the proportion of HIV incidence due to contaminated injections should, in many cases, be substantially modified in light of age-stratified incidence and injection data, resulting in improved (posterior) estimates. Applying the method to data from rural southwest Uganda, we show that the highest estimates of the proportion of incidence due to injections are reduced from 15.5% (95% credible interval) (0.7%, 44.9%) to 5.2% (0.5%, 17.0%) if random mixing is assumed, and from 14.6% (0.7%, 42.5%) to 11.8% (1.2%, 32.5%) under assortative mixing. Lower, and more widely accepted, estimates remain largely unchanged, between 1% and 3% (0.1-6.3%). Although important uncertainty remains, our analysis shows that in rural Uganda, contaminated injections are unlikely to account for a large proportion of HIV incidence. This result is likely to be generalizable to many other populations in sub-Saharan Africa.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Gisselquist DP. Int J STD AIDS. 2002;13:152–159. - PubMed
-
- Gisselquist D, Rothenberg R, Potterat J, Drucker E. Int J STD AIDS. 2002;13:657–666. - PubMed
-
- Hauri A, Armstrong G, Hutin Y. Int J STD AIDS. 2004;15:7–16. - PubMed
-
- Baggaley RF, Boily MC, White RG, Alary M. AIDS. 2006;20:805–812. - PubMed
-
- Schmid GP, Buve A, Mugyenyi P, Garnett GP, Hayes RJ, Williams BG, Calleja JG, De Cock KM, Whitworth JA, Kapiga SH, et al. Lancet. 2004;363:482–488. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
