

A prospective randomized controlled trial of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer
- PMID: 17522511
- PMCID: PMC1876970
- DOI: 10.1097/01.sla.0000259219.08209.36
A prospective randomized controlled trial of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer
Abstract
Objective: A prospective randomized controlled trial (RCT) of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer.
Aims: This study evaluates the use of a multimodal package in colorectal cancer surgery in the context of an RCT.
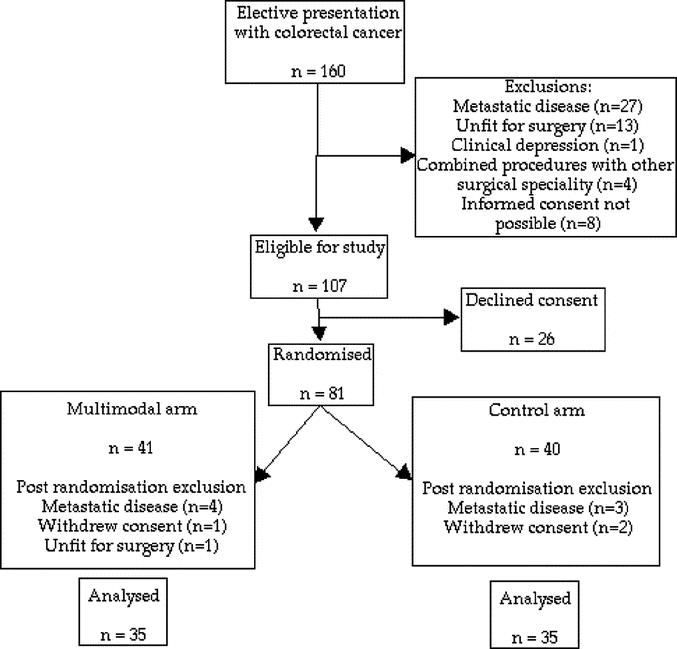
Methods: Patients for elective resection for colorectal cancer were offered trial entry. Participants were stratified by sex and requirement for a total mesorectal excision and centrally randomized. Multimodal patients received intravenous fluid restriction, unrestricted oral intake with prokinetic agents, early ambulation, and fixed regimen epidural analgesia. Control patients received intravenous fluids to prevent oliguria, restricted oral intake until return of bowel motility, and weaning regimen epidural analgesia. Adherence to both regimens was reinforced using a daily checklist and protocol guidance sheets. Discharge decision was made using pre-agreed criteria. The primary endpoint was postoperative stay, and achievement of independence milestones. Secondary endpoints were postoperative complications, readmission rates, and mortality. Analysis was by intention to treat.
Results: Seventy patients were recruited. Approximately one fourth underwent TME. Median ages were similar (69.3 vs. 73.0 years). The median stay was significantly reduced in the multimodal group (5 vs. 7 days; P < 0.001, Mann-Whitney U test). Patients in the control arm were 2.5 times as likely to require a postoperative stay of more than 5 days. Patients in the multimodal group had less cardiorespiratory and anastomotic complications but more readmissions. There were 2 deaths, both controls.
Conclusions: This RCT provides level 1b evidence that a multimodal management protocol can significantly reduce postoperative stay following colorectal cancer surgery. Morbidity and mortality are not increased.
References
-
- Basse L, Thorbol JE, Lossl K, et al. Colonic surgery with accelerated rehabilitation or conventional care. Dis Colon Rectum. 2004;47:271–277; discussion 277–278. - PubMed
-
- Hjort Jakobsen D, Sonne E, Basse L, et al. Convalescence after colonic resection with fast-track versus conventional care. Scand J Surg. 2004;93:24–28. - PubMed
-
- Kehlet H, Mogensen T. Hospital stay of 2 days after open sigmoidectomy with a multimodal rehabilitation programme. Br J Surg. 1999;86:227–230. - PubMed
-
- Gatt M, Anderson AD, Reddy BS, et al. Randomized clinical trial of multimodal optimization of surgical care in patients undergoing major colonic resection. Br J Surg. 2005;92:1354–1362. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
