

Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management
- PMID: 17522514
- PMCID: PMC1876946
- DOI: 10.1097/01.sla.0000256391.05233.aa
Disconnect between incidence of nonperforated and perforated appendicitis: implications for pathophysiology and management
Abstract
Objective: Appendicitis has been declining in frequency for several decades. During the past 10 years, its preoperative diagnosis has been made more reliable by improved computed tomography (CT) imaging. Thresholds for surgical exploration have been lowered by the increased availability of laparoscopic exploration. These innovations should influence the number of appendectomies performed in the United States. We analyzed nationwide hospital discharge data to study the secular trends in appendicitis and appendectomy rates.
Methods: All appendicitis and appendiceal operations reported to the National Hospital Discharge Survey (NHDS) 1970-2004 were classified as perforated, nonperforated, negative, and incidental appendectomies and analyzed over time and by various demographic measures. Secular trends in the population-based incidence rates of nonperforated and perforated appendicitis and negative and incidental appendectomy were examined.
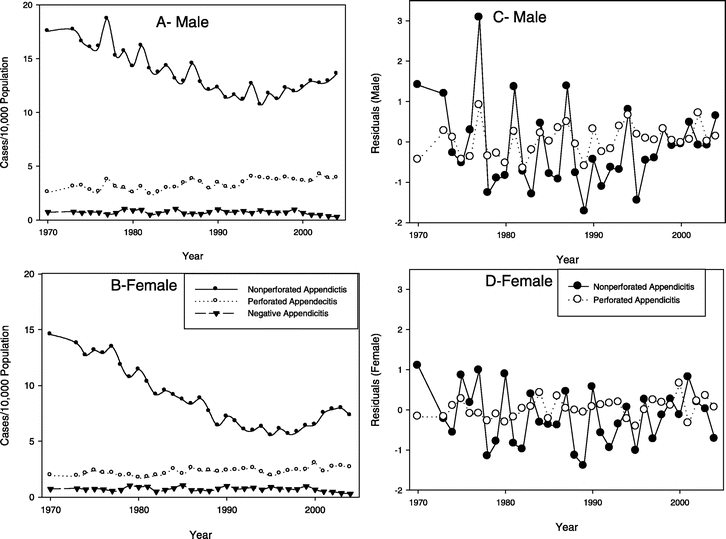
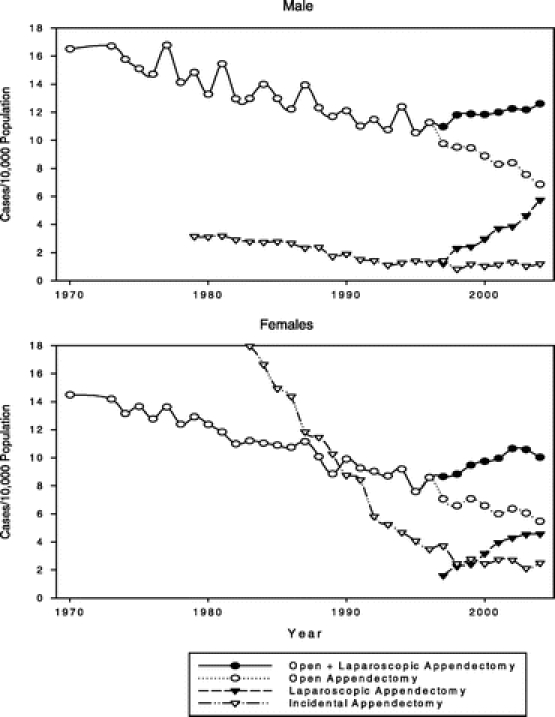
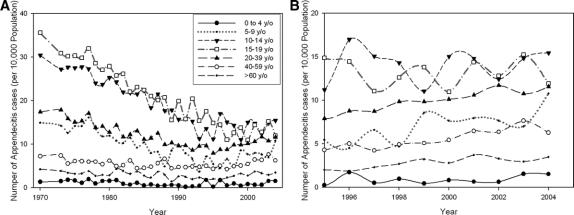
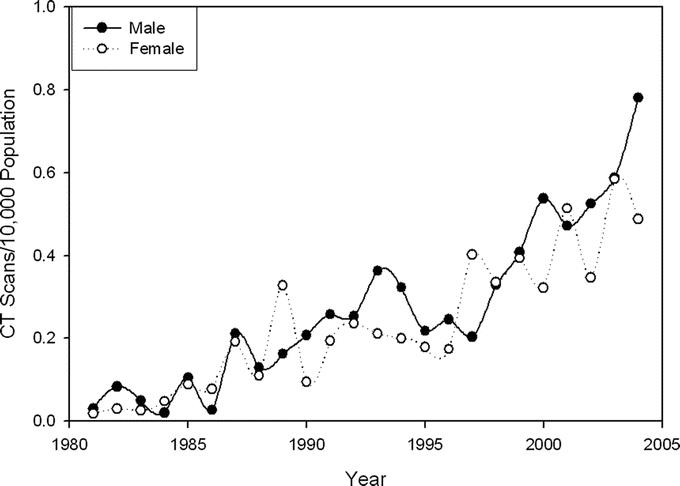
Results: Nonperforated appendicitis rates decreased between 1970 and 1995 but increased thereafter. The 25-year decreasing trend was accounted for almost entirely by a decreasing incidence in the 10-19 year age group. The rise after 1995 occurred in all age groups above 5 years and paralleled increasing rates of CT imaging and laparoscopic surgery on the appendix. Since 1995 the negative appendectomy rate has been falling, especially in women, and incidental appendectomies, frequent in prior decades, have been rarely performed. Despite these large changes, the rate of perforated appendicitis has increased steadily over the same period. Although perforated and nonperforated appendicitis rates were correlated in men, they were not significantly correlated in women nor were there significant negative correlations between perforated and negative appendectomy rates.
Conclusion: The 25-year decline in nonperforated appendicitis and the recent increase in appendectomies coincident with more frequent use of CT imaging and laparoscopic appendectomies did not result in expected decreases in perforation rates. Similarly, time series analysis did not find a significant negative relationship between negative appendectomy and perforation rates. This disconnection of trends suggests that perforated and nonperforated appendicitis may have different pathophysiologies and that nonoperative management with antibiotic therapy may be appropriate for some initially nonperforated cases. Further efforts should be directed at identifying preoperative characteristics associated with nonperforating appendicitis that may eventually allow surgeons to defer operation for those cases of nonperforating appendicitis that have a low perforation risk.
Figures
Comment in
-
Should we disconnect perforated and nonperforated appendicitis in children?Ann Surg. 2008 Mar;247(3):553-4; author reply 554. doi: 10.1097/SLA.0b013e3181661790. Ann Surg. 2008. PMID: 18376203 No abstract available.
-
Nonperforated versus perforating appendicitis.Ann Surg. 2008 Mar;247(3):554; author reply 554-5. doi: 10.1097/SLA.0b013e31816617b8. Ann Surg. 2008. PMID: 18376207 No abstract available.
References
-
- National Center for Health Statistics. Ambulatory and Inpatient Procedures in the United States, 1996. National Center for Health Statistics Series 13[No. 139]. 2004. - PubMed
-
- Larsson PG, Henriksson G, Olsson M, et al. Laparoscopy reduces unnecessary appendicectomies and improves diagnosis in fertile women. A randomized study. Surg Endosc. 2001;15:200–202. - PubMed
-
- Fitz RH. Perforating inflammation of the vermiform appendix with special reference to its early diagnosis and treatment. Trans Assoc Am Physicians. 1886;1:107–144.
-
- Campbell MR, Johnston SL III, Marshburn T, et al. Nonoperative treatment of suspected appendicitis in remote medical care environments: implications for future spaceflight medical care. J Am Coll Surg. 2004;198:822–830. - PubMed
-
- Coldrey E. Five years of conservative treatment of acute appendicitis. J Int Coll Surg. 1959;32:255–261.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
