

Staging of hepatocellular carcinoma: assessment of the Japanese TNM and AJCC/UICC TNM systems in a cohort of 13,772 patients in Japan
- PMID: 17522517
- PMCID: PMC1876960
- DOI: 10.1097/01.sla.0000254368.65878.da
Staging of hepatocellular carcinoma: assessment of the Japanese TNM and AJCC/UICC TNM systems in a cohort of 13,772 patients in Japan
Abstract
Objective: The aims of this study were to present evidence to develop and validate the Japanese Tumor-Node-Metastasis (TNM) staging system for primary liver cancer and to compare its discriminatory ability and predictive power with those of Vauthey's simplified staging, which was adopted as the TNM staging system of the American Joint Committee on Cancer (AJCC)/International Union Against Cancer (UICC).
Summary background data: Among many staging systems for hepatocellular carcinoma, the Japanese TNM staging system and the AJCC/UICC staging system were developed based on a survival analysis of surgical patients. These 2 staging systems have not been compared in large series.
Methods: The Liver Cancer Study Group of Japan (LCSGJ) prospectively collected clinicopathologic data of 63,736 patients with primary liver cancer from 1995 to 2001. Among them, 13,772 patients received curative hepatic resection. Based on univariate and multivariate survival analyses, the Japanese TNM staging system was developed. The accuracy of the Japanese TNM staging system for predicting patient survival was compared with that of the AJCC/UICC staging system using the cross-validation method.
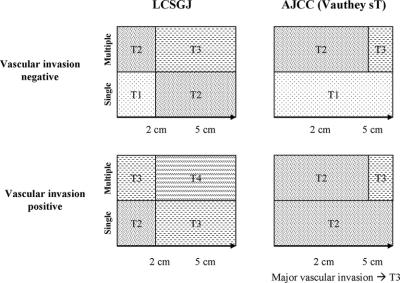
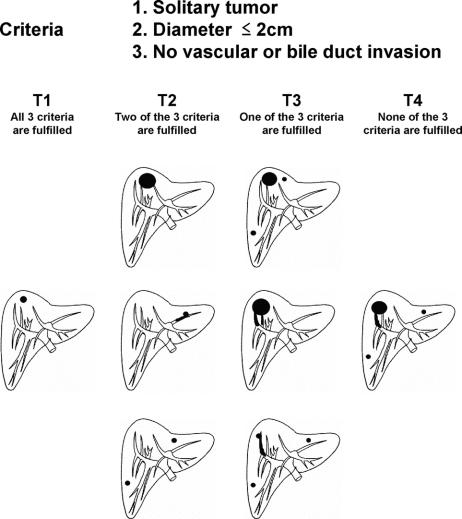
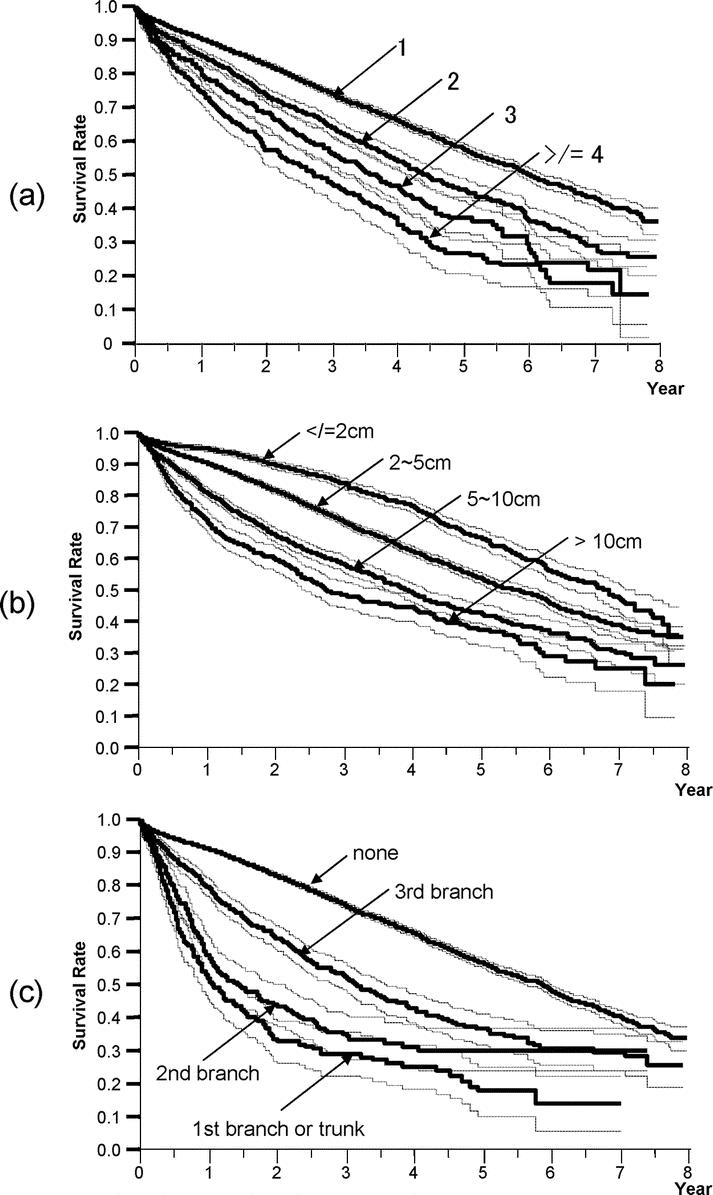
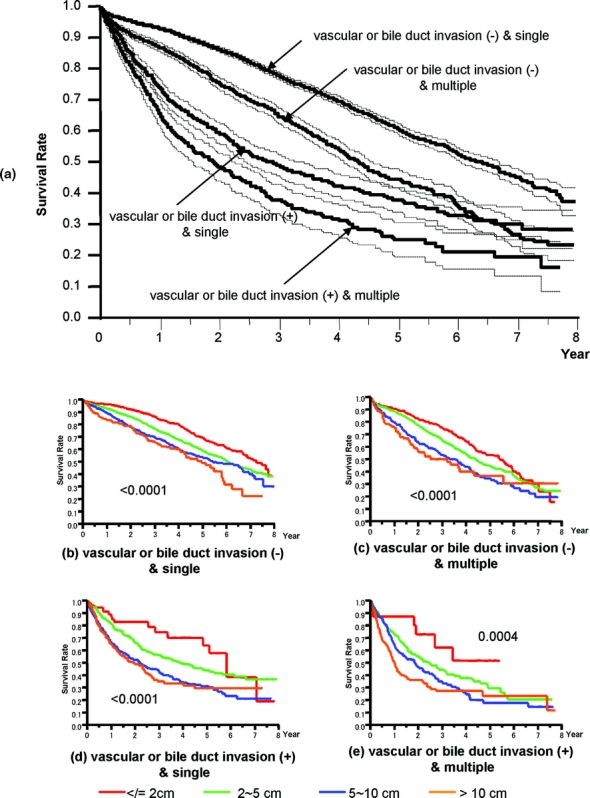
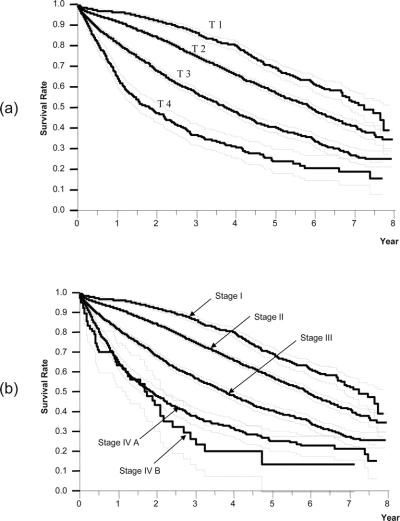
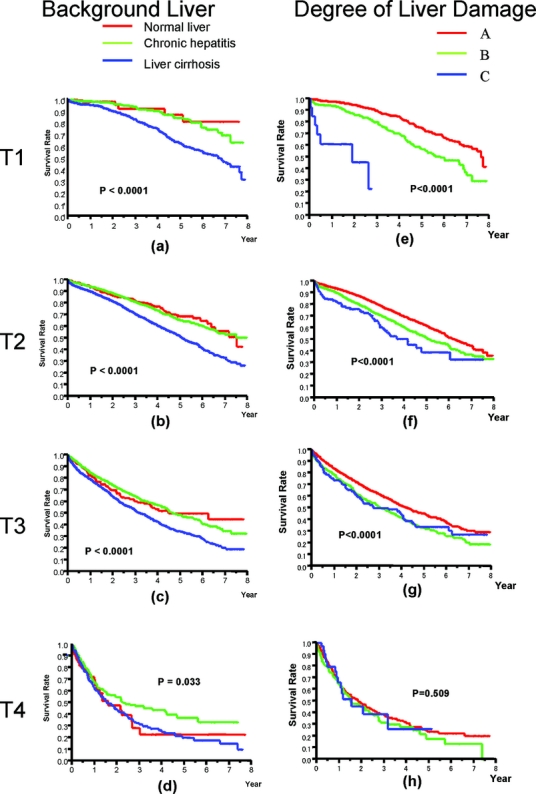
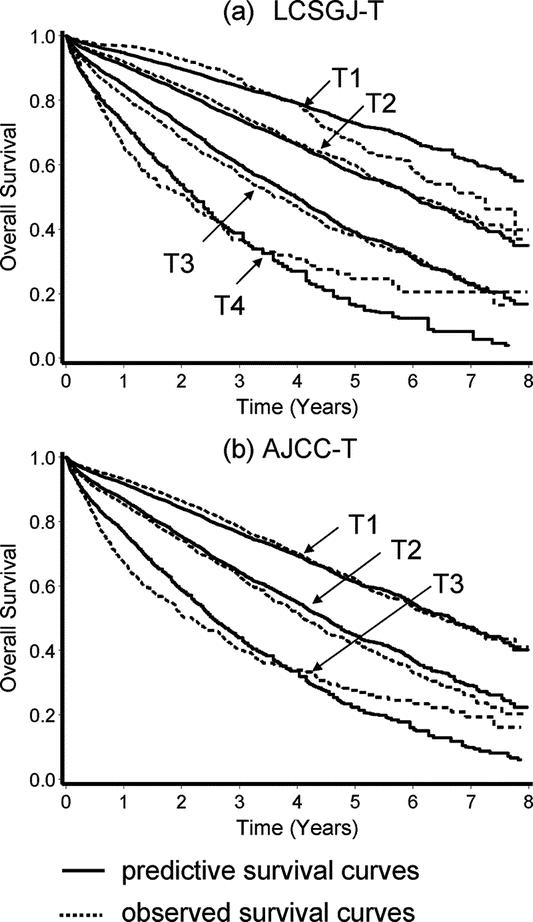
Results: The independent prognostic factors (relative risk; 95% confidence interval) were vascular or bile duct invasion (1.36;1.29-1.43), liver cirrhosis (1.26;1.20-1.32), diameter (< or =2 cm or >2 cm) (1.21;1.14-1.28), alpha-fetoprotein (1.20;1.15-1.25), single/multiple (1.18;1.12-1.23), liver damage (1.15;1.10-1.20), hepatic involvement (1.14;1.09-1.19), histologic differentiation (1.14;1.08-1.20), gross classification (1.13;1.08-1.18), and esophageal varices (1.07;1.02-1.13). Based on these results, 3 criteria (vascular or bile duct invasion, diameter, and single/multiple) were selected. Patients with none of these 3 factors were considered T1, and those with 1, 2, and 3 factors were T2, T3, and T4, respectively. The number of patients and 5-year survival rates for T1, T2, T3, and T4 were 2078, 70%; 6853, 58%; 3021, 41%; and 582, 24% (P < 0.0001), respectively, while those for the AJCC-T were 8457, 61% in T1, 2888, 46% in T2, and 1189, 30% in T3 (P < 0.0001). While both the LCSGJ-T and the AJCC-T had good discriminating ability, the former was significantly superior (P = 0.0007).
Conclusions: Our findings support the development of LCSG stage. While both staging systems allow for the clear stratification of patients into prognostic groups, the LCSGJ staging may be more appropriate for stratifying patients with early-stage HCC.
Figures
References
-
- Arii S, Yamaoka Y, Futagawa S, et al. Results of surgical and nonsurgical treatment for small-sized hepatocellular carcinomas: a retrospective and nationwide survey in Japan. The Liver Cancer Study Group of Japan. Hepatology. 2000;32:1224–1229. - PubMed
-
- Okuda K, Ohtsuki T, Obata H, et al. Natural history of hepatocellular carcinoma and prognosis in relation to treatment: study of 850 patients. Cancer. 1985;56:918–928. - PubMed
-
- Anonymous. A new prognostic system for hepatocellular carcinoma: a retrospective study of 435 patients. The Cancer of the Liver Italian Program (CLIP) investigators. Hepatology. 1998;28:751–755. - PubMed
-
- Llovet JM, Bru C, Bruix J. Prognosis of hepatocellular carcinoma: the BCLC staging classification. Semin Liver Dis. 1999;19:329–338. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
