

Causes of death in U.S. Special Operations Forces in the global war on terrorism: 2001-2004
- PMID: 17522526
- PMCID: PMC1876965
- DOI: 10.1097/01.sla.0000259433.03754.98
Causes of death in U.S. Special Operations Forces in the global war on terrorism: 2001-2004
Abstract
Background: Effective combat trauma management strategies depend upon an understanding of the epidemiology of death on the battlefield.
Methods: A panel of military medical experts reviewed photographs and autopsy and treatment records for all Special Operations Forces (SOF) who died between October 2001 and November 2004 (n = 82). Fatal wounds were classified as nonsurvivable or potentially survivable. Training and equipment available at the time of injury were taken into consideration. A structured analysis was conducted to identify equipment, training, or research requirements for improved future outcomes.
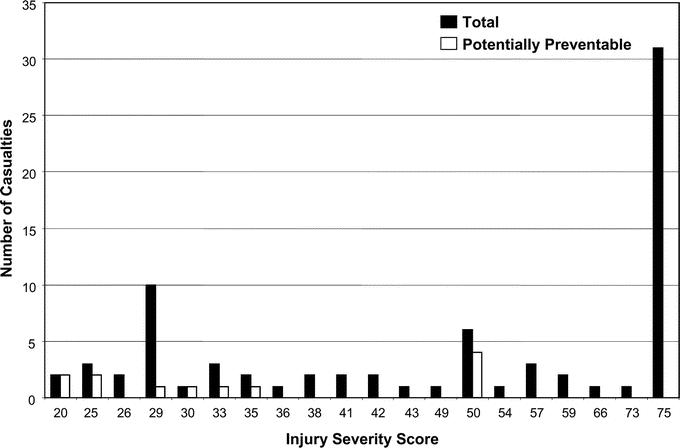
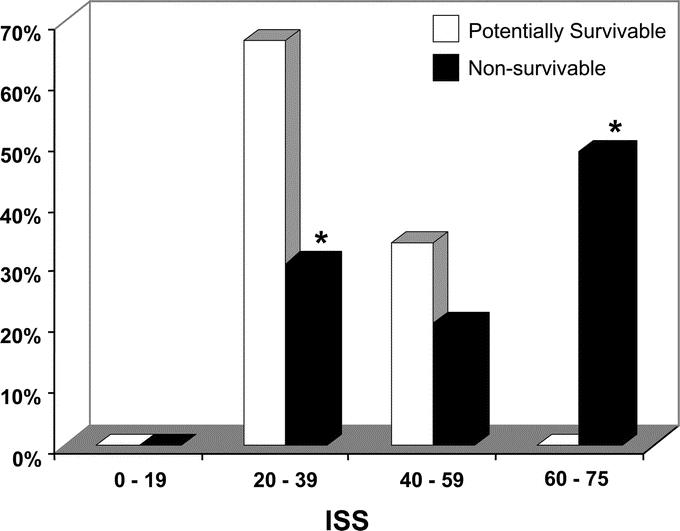
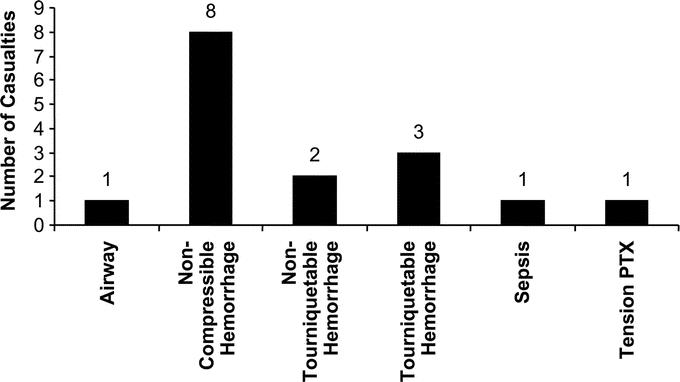
Results: Five (6%) of 82 casualties had died in an aircraft crash, and their bodies were lost at sea; autopsies had been performed on all other 77 soldiers. Nineteen deaths, including the deaths at sea were noncombat; all others were combat related. Deaths were caused by explosions (43%), gunshot wounds (28%), aircraft accidents (23%), and blunt trauma (6%). Seventy of 82 deaths (85%) were classified as nonsurvivable; 12 deaths (15%) were classified as potentially survivable. Of those with potentially survivable injuries, 16 causes of death were identified: 8 (50%) truncal hemorrhage, 3 (19%) compressible hemorrhage, 2 (13%) hemorrhage amenable to tourniquet, and 1 (6%) each from tension pneumothorax, airway obstruction, and sepsis. The population with nonsurvivable injuries was more severely injured than the population with potentially survivable injuries. Structured analysis identified improved methods of truncal hemorrhage control as a principal research requirement.
Conclusions: The majority of deaths on the modern battlefield are nonsurvivable. Improved methods of intravenous or intracavitary, noncompressible hemostasis combined with rapid evacuation to surgery may increase survival.
Figures
References
-
- Cales RH, Trunkey DD. Preventable trauma deaths: a review of trauma care systems development. JAMA. 1985;254:1059–1063. - PubMed
-
- Dubois RW, Brook RH. Preventable deaths: who, how often, and why? Ann Intern Med. 1988;109:582–589. - PubMed
-
- Bellamy RF, Maningas PA, Vayer JS. Epidemiology of trauma: military experience. Ann Emerg Med. 1986;15:1384–1388. - PubMed
-
- Blood CG, Puyana JC, Pitlyk PJ, et al. An assessment of the potential for reducing future combat deaths through medical technologies and training. J Trauma. 2002;53:1160–1165. - PubMed
-
- Carey ME. Analysis of wounds incurred by U.S. Army Seventh Corps personnel treated in Corps hospitals during Operation Desert Storm, February 20 to March 10, 1991. J Trauma. 1996;40(suppl 3):165–169. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
