

Maltreatment of Strongyloides infection: case series and worldwide physicians-in-training survey
- PMID: 17524758
- PMCID: PMC1950578
- DOI: 10.1016/j.amjmed.2006.05.072
Maltreatment of Strongyloides infection: case series and worldwide physicians-in-training survey
Abstract
Background: Strongyloidiasis infects hundreds of millions of people worldwide and is an important cause of mortality from intestinal helminth infection in developed countries. The persistence of infection, increasing international travel, lack of familiarity by health care providers, and potential for iatrogenic hyperinfection all make strongyloidiasis an important emerging infection.
Methods: Two studies were performed. A retrospective chart review of Strongyloides stercoralis cases identified through microbiology laboratory records from 1993-2002 was conducted. Subsequently, 363 resident physicians in 15 training programs worldwide were queried with a case scenario of strongyloidiasis, presenting an immigrant with wheezing and eosinophilia. The evaluation focused on resident recognition and diagnostic recommendations.
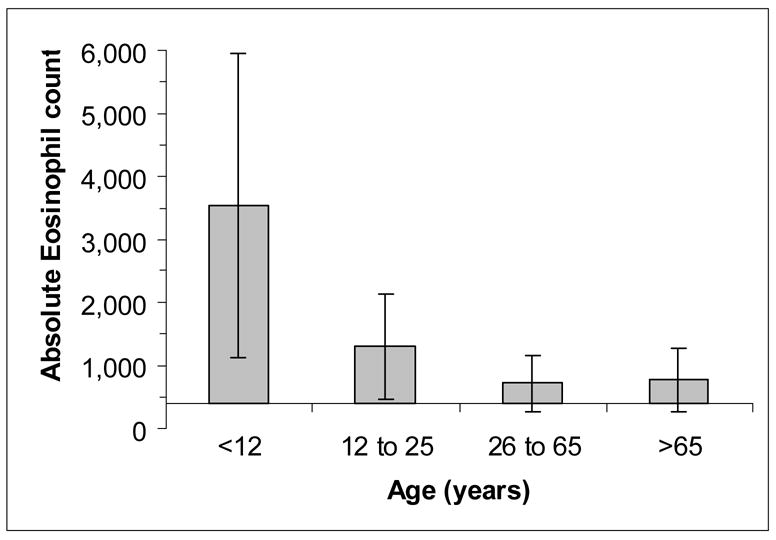
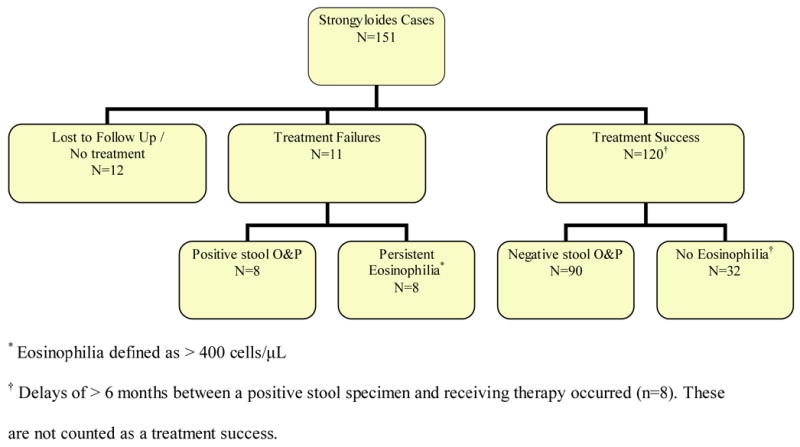
Results: In 151 strongyloidiasis cases, stool ova and parasite sensitivity is poor (51%), and eosinophilia (>5% or >400 cells/microL) commonly present (84%). Diagnosis averaged 56 months (intra-quartile range: 4-72 months) after immigration. Presenting complaints were nonspecific, although 10% presented with wheezing. Hyperinfection occurred in 5 patients prescribed corticosteroids, with 2 deaths. Treatment errors occurred more often among providers unfamiliar with immigrant health (relative risk of error: 8.4; 95% confidence interval, 3.4-21.0; P <.001). When presented with a hypothetical case scenario, US physicians-in-training had poor recognition (9%) of the need for parasite screening and frequently advocated empiric corticosteroids (23%). International trainees had superior recognition at 56% (P <.001). Among US trainees, 41% were unable to choose any parasite causing pulmonary symptoms.
Conclusions: Strongyloidiasis is present in US patients. Diagnostic consideration should occur with appropriate exposure, nonspecific symptoms including wheezing, or eosinophilia (>5% relative or >400 eosinophils/microL). US residents' helminth knowledge is limited and places immigrants in iatrogenic danger. Information about Strongyloides should be included in US training and continuing medical education programs.
Figures
References
-
- Liu LX, Weller PF. Strongyloides and other intestinal nematode infections. Infect Dis Clin North Am. 1993;7:655–82. - PubMed
-
- Genta RM. Global prevalence of strongyloidiasis: critical review with epidemiologic insights into the prevention of disseminated disease. Rev Infect Dis. 1989;11:755–67. - PubMed
-
- Nutman TB, Ottesen EA, Ieng S, et al. Eosinophilia in Southeast Asian refugees: evaluation at a referral center. J Infect Dis. 1987;155:309–13. - PubMed
-
- Hoffman SL, Barrett-Connor E, Norcross W, Nguyen D. Intestinal parasites in Indochinese immigrants. Am J Trop Med Hyg. 1981;30:340–43. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
