

Clinical characteristics and outcome of Candida keratitis
- PMID: 17524775
- PMCID: PMC2040331
- DOI: 10.1016/j.ajo.2007.02.016
Clinical characteristics and outcome of Candida keratitis
Abstract
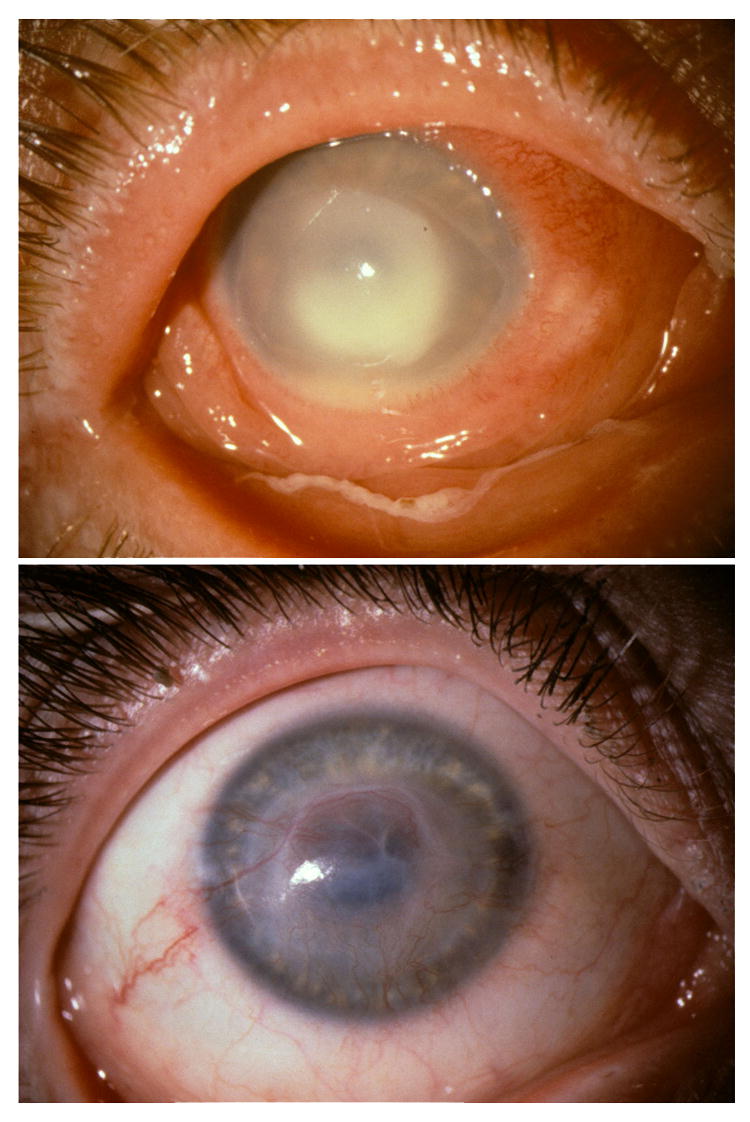
Purpose: To characterize the clinical features and therapeutic outcome of Candida keratitis.
Design: Retrospective, observational case series.
Methods: We reviewed 26 patients treated for Candida keratitis, including two with recurrent keratitis and one with bilateral infection.
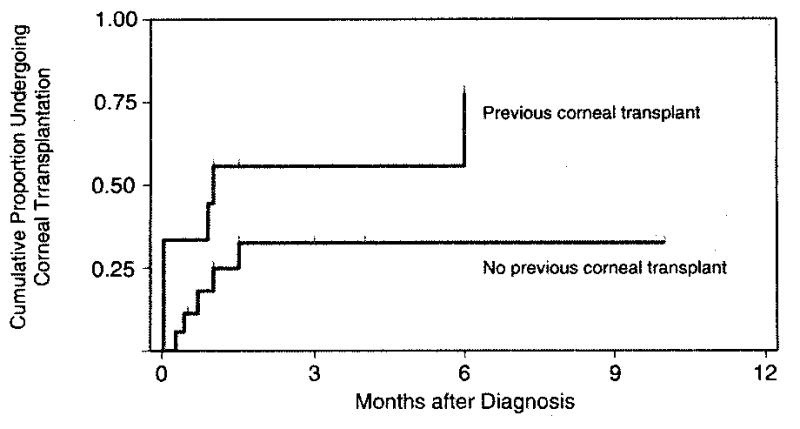
Results: Of 29 keratitis episodes resulting from Candida albicans (n = 20) or Candida parapsilosis (n = 9), 16 (55%) complicated chronic ocular surface disease, and nine (31%) followed previous keratoplasty. Only two were clinically suspected to have keratomycosis at initial presentation, and 21 (72%) used antibacterial therapy before corneal scrapings. Reconstructive keratoplasty occurred more often in previously grafted eyes (P = .03). Visual outcome was 20/60 or better in six (100%) medically treated eyes with good presenting visual acuity but in only five eyes (24%) with worse initial vision (P = .002).
Conclusions: Candida keratitis is an opportunistic infection of a compromised cornea that often is misdiagnosed initially and, despite antifungal therapy, occasionally requires corneal grafting.
Figures
References
-
- Sykes E. Fungal infections of the cornea. Tex State J Med. 1946;42:330–332. - PubMed
-
- Behrens-Baumann W. Mycosis of the Eye and its Adnexa. Basel: S Karger; 1999. p. 80.
-
- Kelly L, Pavan-Langston D, Baker A. Keratomycosis in a New England referral center: spectrum of pathogenic organisms and predisposing factors. In: Bialasiewicz AA, Schaal KP, editors. Infectious Diseases of the Eye. Buren: Æolus Press; 1994. pp. 184–190.
-
- Tanure MAG, Cohen EJ, Sudesh S, Rapuano CJ, Laibson PR. Spectrum of fungal keratitis at Wills Eye Hospital, Philadelphia, Pennsylvania. Cornea. 2000;19:307–312. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
